

Inequity in Access to Transplantation in the United Kingdom
- PMID: 32467306
- PMCID: PMC7274279
- DOI: 10.2215/CJN.11460919
Inequity in Access to Transplantation in the United Kingdom
Abstract
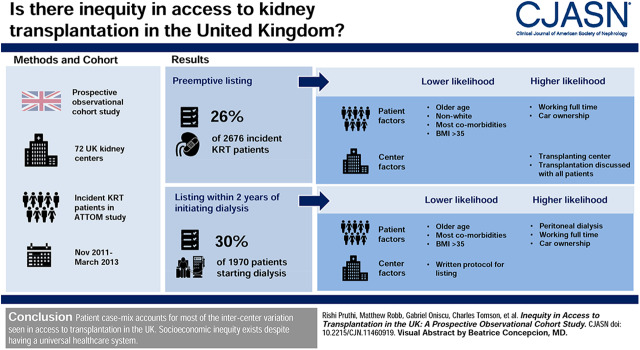
Background and objectives: Despite the presence of a universal health care system, it is unclear if there is intercenter variation in access to kidney transplantation in the United Kingdom. This study aims to assess whether equity exists in access to kidney transplantation in the United Kingdom after adjustment for patient-specific factors and center practice patterns.
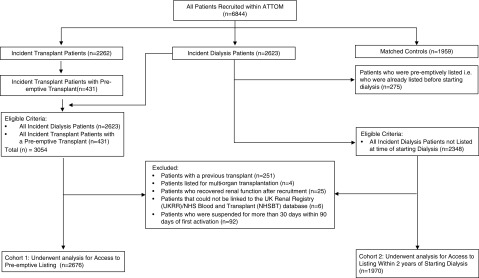
Design, setting, participants, & measurements: In this prospective, observational cohort study including all 71 United Kingdom kidney centers, incident RRT patients recruited between November 2011 and March 2013 as part of the Access to Transplantation and Transplant Outcome Measures study were analyzed to assess preemptive listing (n=2676) and listing within 2 years of starting dialysis (n=1970) by center.
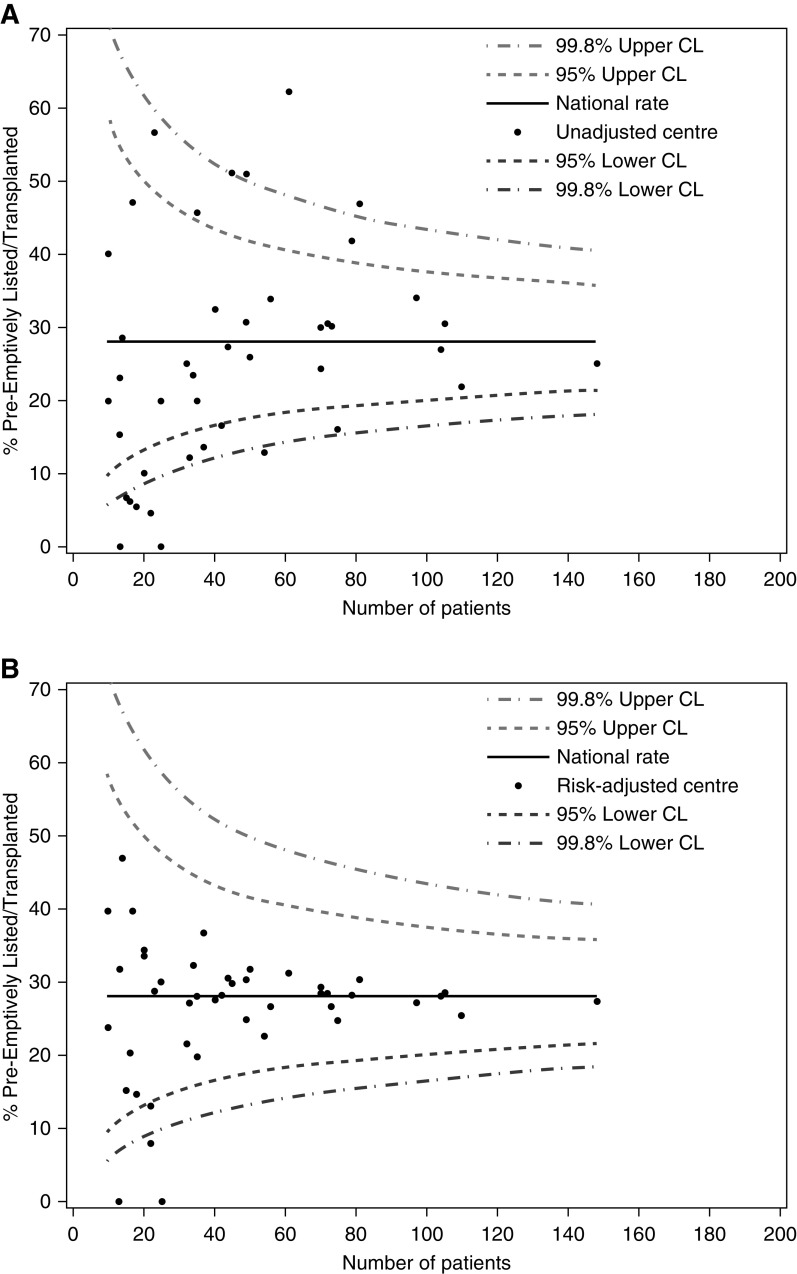
Results: Seven hundred and six participants (26%) were listed preemptively, whereas 585 (30%) were listed within 2 years of commencing dialysis. The interquartile range across centers was 6%-33% for preemptive listing and 25%-40% for listing after starting dialysis. Patient factors, including increasing age, most comorbidities, body mass index >35 kg/m2, and lower socioeconomic status, were associated with a lower likelihood of being listed and accounted for 89% and 97% of measured intercenter variation for preemptive listing and listing within 2 years of starting dialysis, respectively. Asian (odds ratio, 0.49; 95% confidence interval, 0.33 to 0.72) and Black (odds ratio, 0.43; 95% confidence interval, 0.26 to 0.71) participants were both associated with reduced access to preemptive listing; however Asian participants were associated with a higher likelihood of being listed after starting dialysis (odds ratio, 1.42; 95% confidence interval, 1.12 to 1.79). As for center factors, being registered at a transplanting center (odds ratio, 3.1; 95% confidence interval, 2.36 to 4.07) and a universal approach to discussing transplantation (odds ratio, 1.4; 95% confidence interval, 1.08 to 1.78) were associated with higher preemptive listing, whereas using a written protocol was associated negatively with listing within 2 years of starting dialysis (odds ratio, 0.7; 95% confidence interval, 0.58 to 0.9).
Conclusions: Patient case mix accounts for most of the intercenter variation seen in access to transplantation in the United Kingdom, with practice patterns also contributing some variation. Socioeconomic inequity exists despite having a universal health care system.
Keywords: African Americans; Body Mass Index; Cohort Studies; Diagnosis-Related Groups; Epidemiology and outcomes; Ethnic Groups; Health Care; Minority Groups; Outcome Assessment; Prospective Studies; Renal Replacement Therapy; Social Class; Universal Health Care; clinical epidemiology; ethnicity; inequity; kidney transplantation; renal dialysis; socio-economic deprivation; transplant waiting list.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Will Universal Access to Health Care Mean Equitable Access to Kidney Transplantation?Clin J Am Soc Nephrol. 2020 Jun 8;15(6):752-754. doi: 10.2215/CJN.03000320. Epub 2020 May 28. Clin J Am Soc Nephrol. 2020. PMID: 32467308 Free PMC article. No abstract available.
References
-
- Public Health England : Chronic kidney disease prevalence model, 2014. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploa.... Accessed September 15, 2019
-
- MacNeill SJ, Ford D, Evans K, Medcalf JF: Chapter 2 UK renal replacement therapy adult prevalence in 2016: National and centre-specific analyses. Nephron 139[Suppl 1]: 47–74, 2018. - PubMed
-
- Gilg J, Methven S, Casula A, Castledine C: UK renal registry 19th annual report: Chapter 1 UK RRT adult incidence in 2015: National and centre-specific analyses. Nephron 137[Suppl 1]: 11–44, 2017. - PubMed
-
- United States Renal Data System : 2017 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2017
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
