

Use of bilobed partial resuscitative endovascular balloon occlusion of the aorta is logistically superior in prolonged management of a highly lethal aortic injury
- PMID: 32467463
- PMCID: PMC7483305
- DOI: 10.1097/TA.0000000000002797
Use of bilobed partial resuscitative endovascular balloon occlusion of the aorta is logistically superior in prolonged management of a highly lethal aortic injury
Abstract
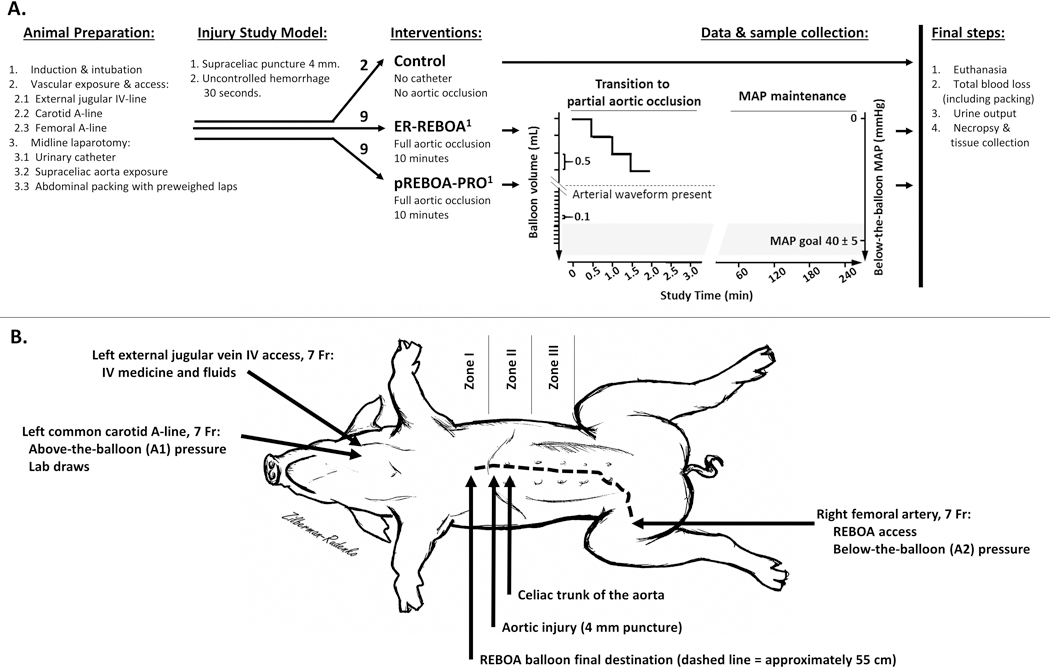
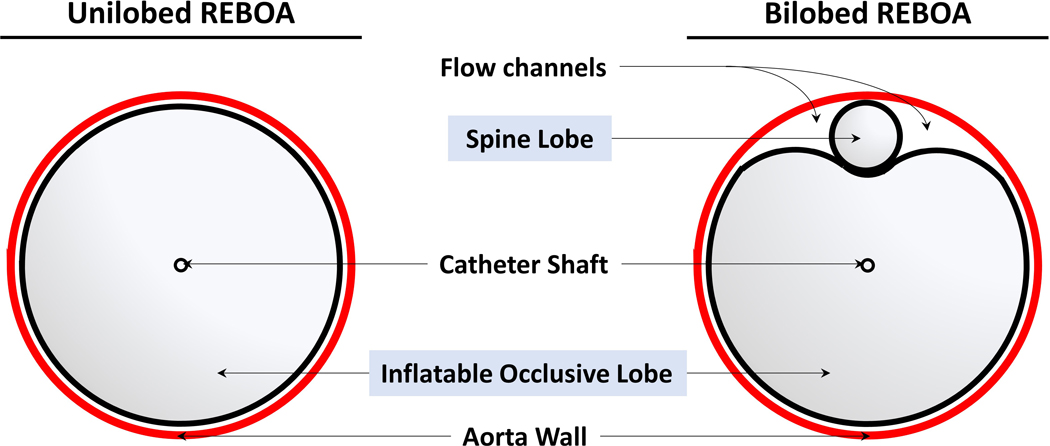
Background: Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a viable technique for management of noncompressible torso hemorrhage. The major limitation of the current unilobed fully occlusive REBOA catheters is below-the-balloon ischemia-reperfusion complications. We hypothesized that partial aortic occlusion with a novel bilobed partial (p)REBOA-PRO would result in the need for less intraaortic balloon adjustments to maintain a distal goal perfusion pressure as compared with currently available unilobed ER-REBOA.
Methods: Anesthetized (40-50 kg) swine randomized to control (no intervention), ER-REBOA, or pREBOA-PRO underwent supraceliac aortic injury. The REBOA groups underwent catheter placement into zone 1 with initial balloon inflation to full occlusion for 10 minutes followed by gradual deflation to achieve and subsequently maintain half of the baseline below-the-balloon mean arterial pressure (MAP). Physiologic data and blood samples were collected at baseline and then hourly. At 4 hours, the animals were euthanized, total blood loss and urine output were recorded, and tissue samples were collected.
Results: Baseline physiologic data and basic laboratories were similar between groups. Compared with control, interventions similarly prolonged survival from a median of 18 minutes to over 240 minutes with comparable mortality trends. Blood loss was similar between partial ER-REBOA (41%) and pREBOA-PRO (51%). Partial pREBOA-PRO required a significantly lower number of intraaortic balloon adjustments (10 ER-REBOA vs. 3 pREBOA-PRO, p < 0.05) to maintain the target below-the-balloon MAP. The partial ER-REBOA group developed significantly increased hypercapnia, fibrin clot formation on TEG, liver inflammation, and IL-10 expression compared with pREBOA-PRO.
Conclusion: In this highly lethal aortic injury model, use of bilobed pREBOA-PRO for a 4-hour partial aortic occlusion was logistically superior to unilobed ER-REBOA. It required less intraaortic balloon adjustments to maintain target MAP and resulted in less inflammation.
Conflict of interest statement
Figures
References
-
- Drake SA, Holcomb JB, Yang Y, Thetford C, Myers L, Brock M, Wolf DA, Cron S, Persse D, McCarthy J, et al. Establishing a Regional Trauma Preventable/Potentially Preventable Death Rate. Ann Surg. 2020;271(2):375–382. - PubMed
-
- Morrison JJ, Stannard A, Rasmussen TE, Jansen JO, Tai NRM, Midwinter MJ. Injury pattern and mortality of noncompressible torso hemorrhage in UK combat casualties. J Trauma Acute Care Surg. 2013;75(2 Suppl 2):S263–268. - PubMed
-
- Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, Mallett O, Zubko T, Oetjen-Gerdes L, Rasmussen TE, et al. Death on the battlefield (2001–2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S431–437. - PubMed
-
- Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, Pons PT. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38(2):185–193. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
