

Barrett's oesophagus and oesophageal adenocarcinoma
- PMID: 32467662
- PMCID: PMC7255890
- DOI: 10.1016/j.mpmed.2019.02.005
Barrett's oesophagus and oesophageal adenocarcinoma
Abstract
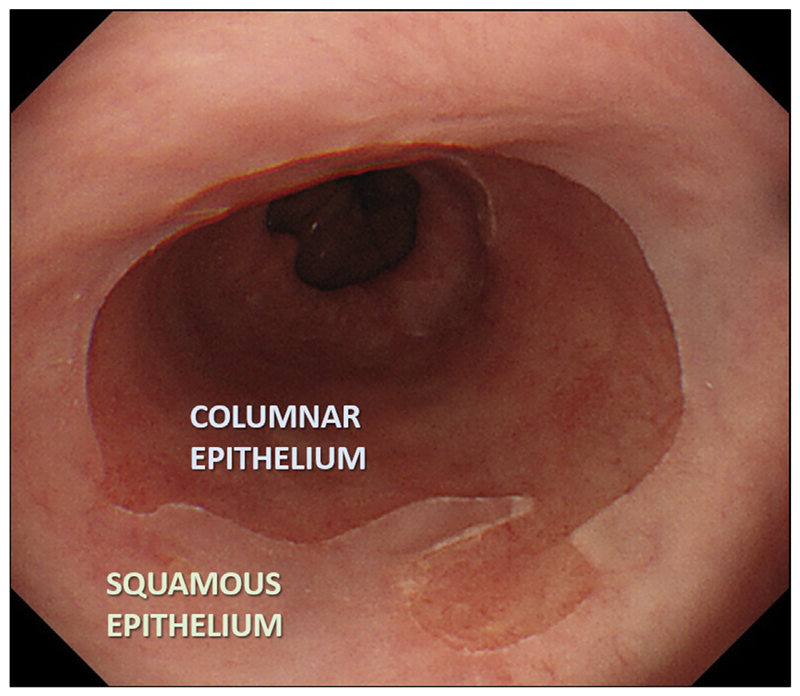
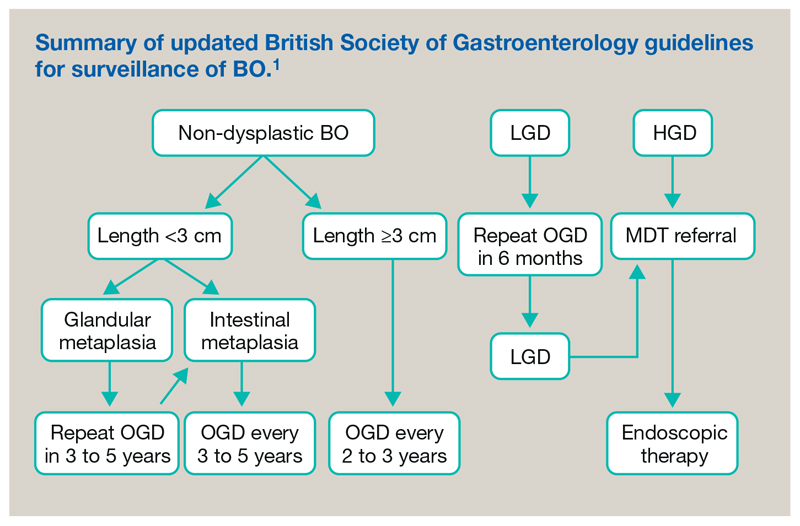
Oesophageal adenocarcinoma (OAC) has increased dramatically in Western countries, including the UK, over the past 30 years. It usually presents de novo, but is often preceded by Barrett's oesophagus (BO), a premalignant condition whereby the normal squamous epithelium is replaced by columnar lined epithelium with intestinal metaplasia. The main risk factors for BO include male sex, obesity and chronic gastro-oesophageal reflux of acid and bile. The estimated annual risk of BO progression is 0.3%, increasing substantially, up to 30%, when dysplasia is present. Endoscopic surveillance is recommended to detect neoplastic changes at an early stage and considerable evidence supports endoscopic treatment for confirmed low- and high-grade dysplasia, and intramucosal adenocarcinoma. Most OACs are diagnosed at a more advanced stage requiring CT-PET assessment and multi-modal treatment. Surgical treatment is performed in specialist centres, increasingly combined with cytotoxic chemotherapy and radiotherapy, involving close liaison between members of the multidisciplinary team. Molecular targeted therapies, such as HER2 and VEGFR-inhibitors, are beginning to penetrate clinical practice, but high molecular heterogeneity has impeded progress. In view of the overall dismal survival (<20%) for advanced OAC, there is renewed interest in screening techniques for early detection and intervention of dysplastic BO.
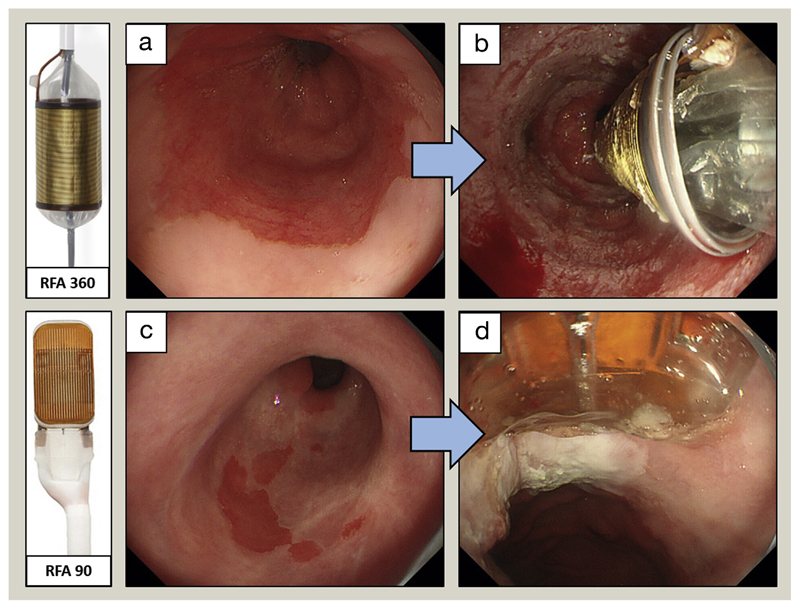
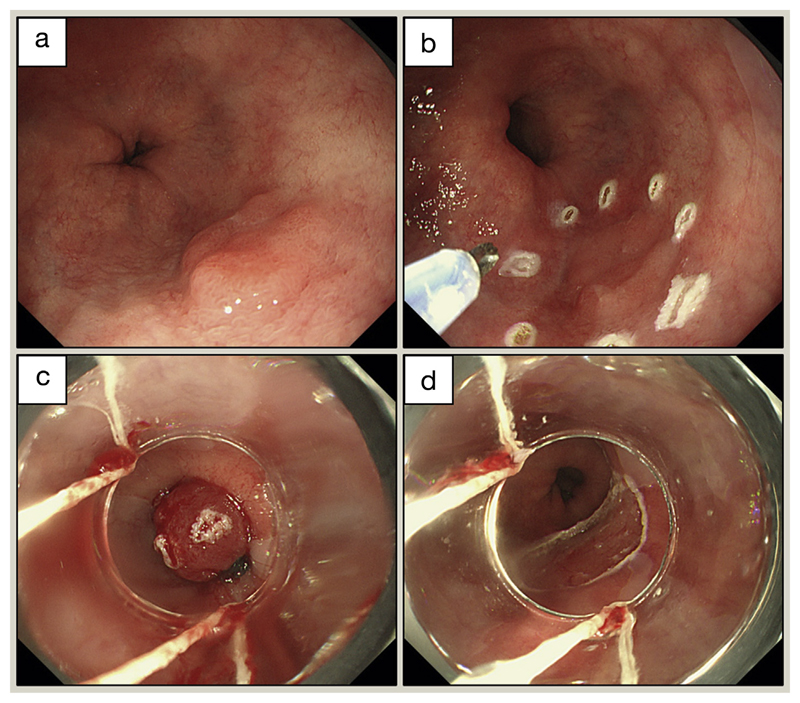
Keywords: Ablation; Barrett’s oesophagus; MRCP; adenocarcinoma; biomarkers; dysphagia; endoscopic mucosal resection; endoscopy; oesophagectomy; radiofrequency; screening; staging; surveillance.
Conflict of interest statement
Competing interests: none declared. Competing interests: Rebecca Fitzgerald developed the Cytosponge-TFF3 test, which has been licensed by the Medical Research Council to Covidien (now Medtronic).
Figures
References
Key References
-
- Fitzgerald RC, di Pietro M, Ragunath K, et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett’s oesophagus. Gut. 2014;63:7–42. - PubMed
-
- Verbeek RE, Leenders M, Ten Kate FJ, et al. Surveillance of Barrett’s esophagus and mortality from esophageal adenocarcinoma: a population-based cohort study. Am J Gastroenterol. 2014;109:1215–22. - PubMed
-
- Coleman HG, Xie SH, Lagergren J. The epidemiology of esophageal adenocarcinoma. Gastroenterol. 2018;154:390–405. - PubMed
Further Reading
-
- Poa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia: a randomized clinical trial. J Am Med Assoc. 2014;311:1209–17. - PubMed
-
- Quante M, Graham TA, Jansen M. Insights into the pathophysiology of esophageal adenocarcinoma. Gastroenterol. 2018;154:406–20. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous