

Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52 816 Patients From 12 Randomized Trials
- PMID: 32468837
- PMCID: PMC7489363
- DOI: 10.1161/CIRCULATIONAHA.120.046786
Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52 816 Patients From 12 Randomized Trials
Abstract
Background: New randomized, controlled trials have become available on oral P2Y12 inhibitors in acute coronary syndrome. We aimed to evaluate current evidence comparing the efficacy and safety profile of prasugrel, ticagrelor, and clopidogrel in acute coronary syndrome by a meta-analysis of randomized controlled trials.
Methods: We performed a network meta-analysis and direct pairwise comparison analysis of efficacy and safety outcomes from 12 randomized controlled trials including a total of 52 816 patients with acute coronary syndrome.
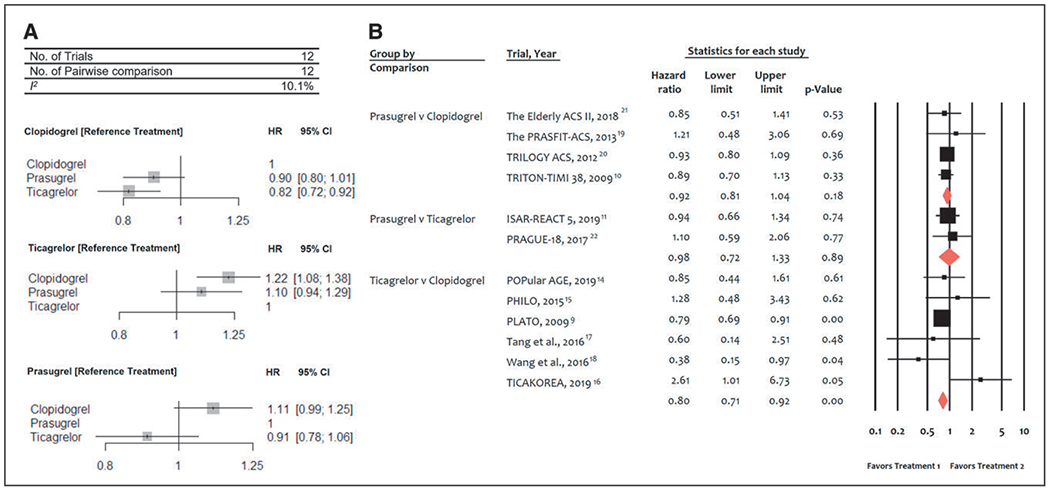
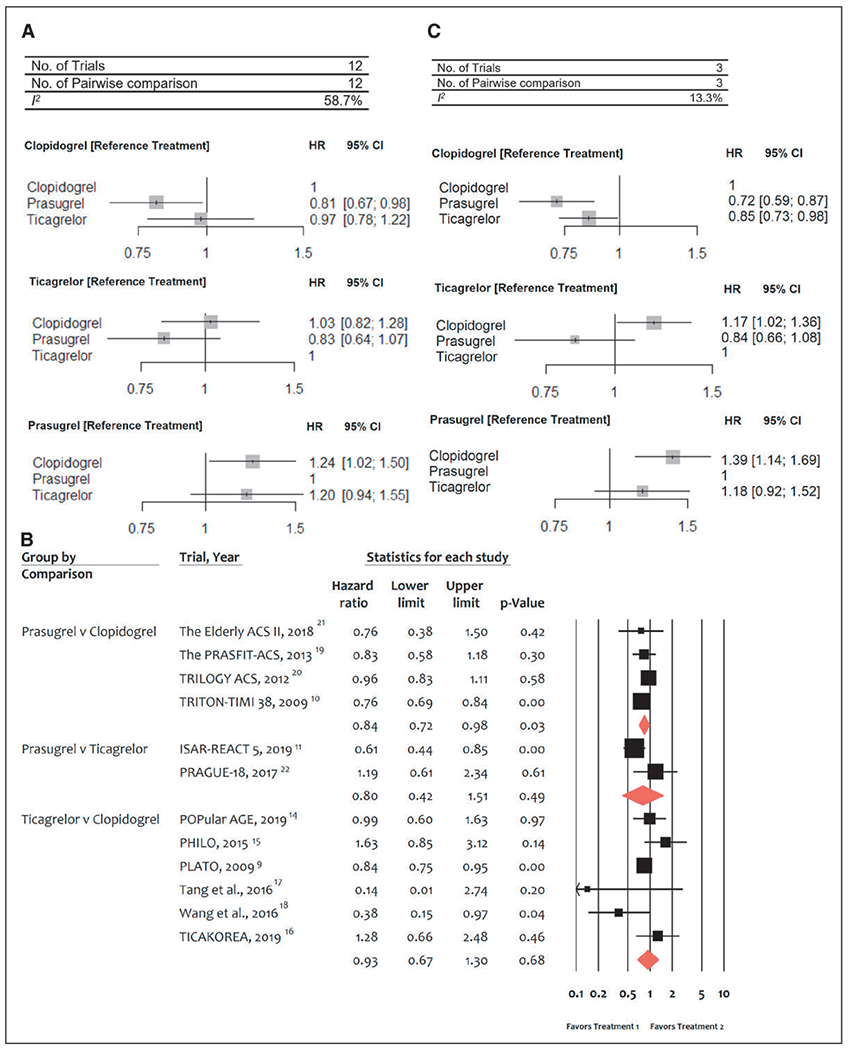
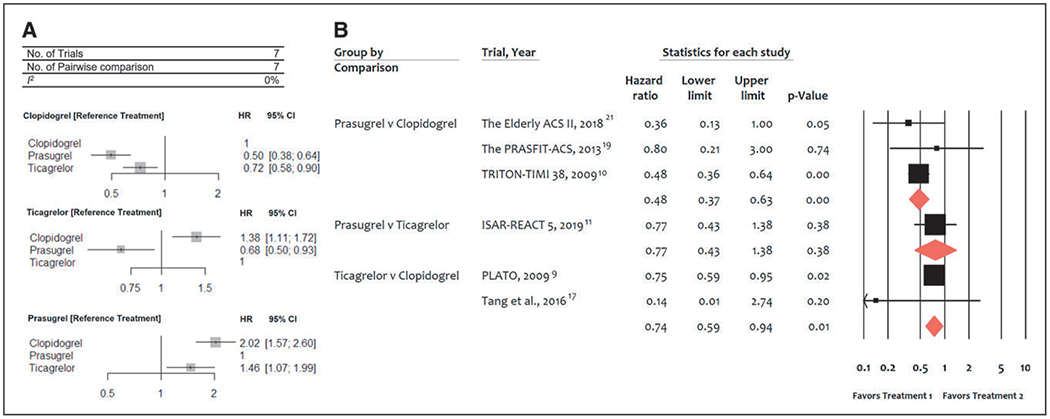
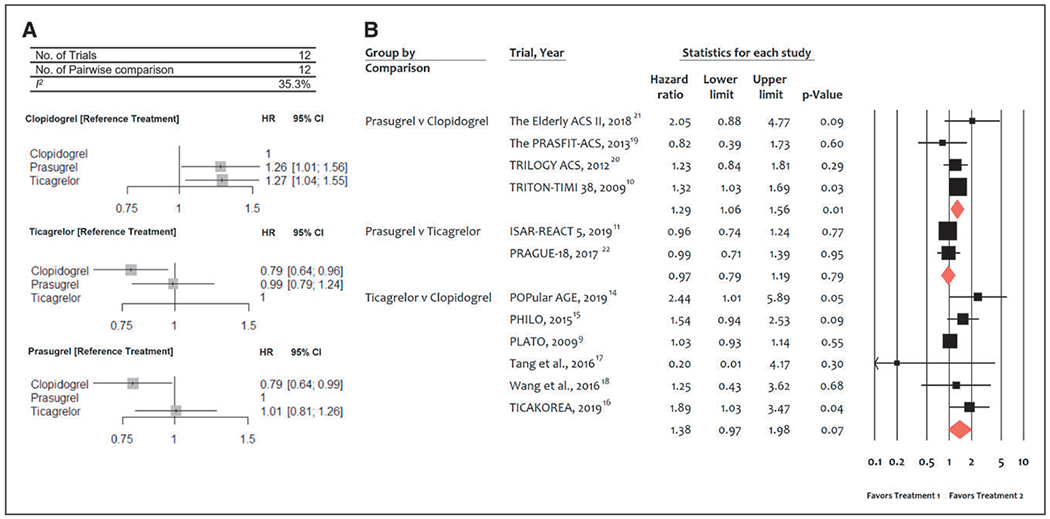
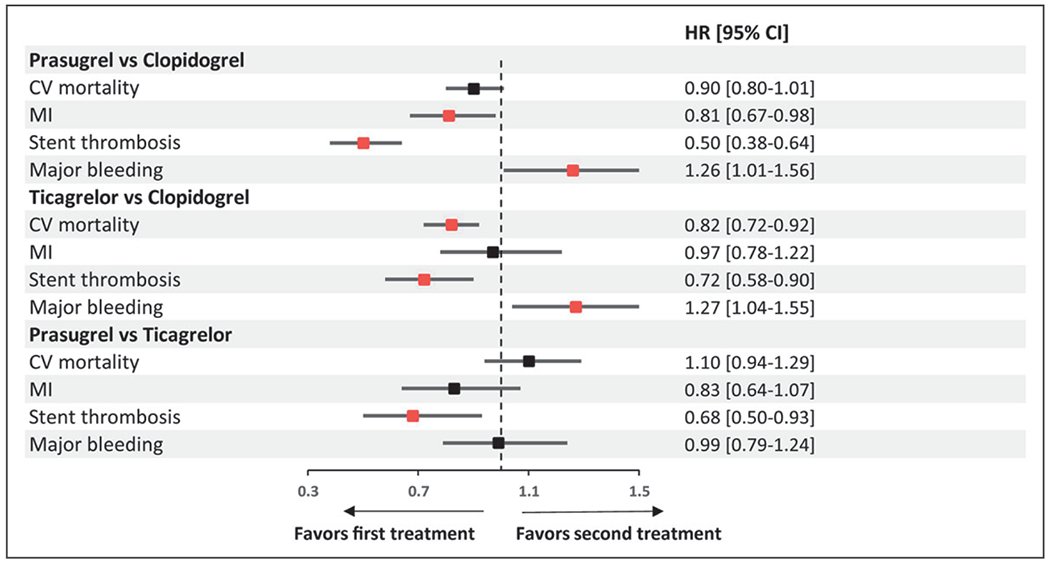
Results: In comparison with clopidogrel, ticagrelor significantly reduced cardiovascular mortality (hazard ratio [HR], 0.82 [95% CI, 0.72-0.92]) and all-cause mortality (HR, 0.83 [95% CI, 0.75-0.92]), whereas there was no statistically significant mortality reduction with prasugrel (HR, 0.90 [95% CI, 0.80-1.01] and HR, 0.92 [95% CI, 0.84-1.02], respectively). In comparison with each other, there were no significant differences in mortality (HR prasugrel versus ticagrelor, 1.10 [95% CI, 0.94-1.29] and 1.12 [95% CI, 0.98-1.28]). In comparison with clopidogrel, prasugrel reduced myocardial infarction (HR, 0.81 [95% CI, 0.67-0.98]), whereas ticagrelor showed no risk reduction (HR, 0.97 [95% CI, 0.78-1.22]). Differences between prasugrel and ticagrelor were not statistically significant. Stent thrombosis risk was significantly reduced by both ticagrelor and prasugrel versus clopidogrel (28%-50% range of reduction). In comparison with clopidogrel, both prasugrel (HR, 1.26 [95% CI, 1.01-1.56]) and ticagrelor (HR, 1.27 [95% CI, 1.04-1.55]) significantly increased major bleeding. There were no significant differences between prasugrel and ticagrelor for all outcomes explored.
Conclusions: Prasugrel and ticagrelor reduced ischemic events and increased bleeding in comparison with clopidogrel. A significant mortality reduction was observed with ticagrelor only. There was no efficacy and safety difference between prasugrel and ticagrelor. Registration: URL: https://www.crd.york.ac.uk/PROSPERO/; Unique identifier: CRD42019155648.
Keywords: P2Y12 protein, human; acute coronary syndrome; meta-analysis.
Figures
Comment in
-
In ACS, ticagrelor and prasugrel each reduce some ischemic events but increase major bleeding vs. clopidogrel.Ann Intern Med. 2020 Oct 20;173(8):JC44. doi: 10.7326/ACPJ202010200-044. Ann Intern Med. 2020. PMID: 33075264
-
Letter by Alkhalil and Kuzemczak Regarding Article, "Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52 816 Patients From 12 Randomized Trials".Circulation. 2021 Feb 9;143(6):e234-e235. doi: 10.1161/CIRCULATIONAHA.120.050967. Epub 2021 Feb 8. Circulation. 2021. PMID: 33555915 No abstract available.
-
Response by Navarese et al to Letters Regarding Article, "Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52 816 Patients From 12 Randomized Trials".Circulation. 2021 Feb 9;143(6):e236-e237. doi: 10.1161/CIRCULATIONAHA.120.051630. Epub 2021 Feb 8. Circulation. 2021. PMID: 33555917 No abstract available.
-
Letter by Kessler et al Regarding Article, "Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52 816 Patients From 12 Randomized Trials".Circulation. 2021 Feb 9;143(6):e230-e231. doi: 10.1161/CIRCULATIONAHA.120.049650. Epub 2021 Feb 8. Circulation. 2021. PMID: 33555921 No abstract available.
-
Letter by Ferracane et al Regarding Article, "Comparative Efficacy and Safety of Oral P2Y12 Inhibitors in Acute Coronary Syndrome: Network Meta-Analysis of 52 816 Patients From 12 Randomized Trials".Circulation. 2021 Feb 9;143(6):e232-e233. doi: 10.1161/CIRCULATIONAHA.120.050472. Epub 2021 Feb 8. Circulation. 2021. PMID: 33555923 No abstract available.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. ; ESC Scientific Document Group. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, et al. ; ESC Scientific Document Group. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267–315. doi: 10.1093/eurheartj/ehv320 - DOI - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139–228. doi: 10.1016/j.jacc.2014.09.017 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
