

Using Virtual Reality to Improve Apathy in Residential Aged Care: Mixed Methods Study
- PMID: 32469314
- PMCID: PMC7380990
- DOI: 10.2196/17632
Using Virtual Reality to Improve Apathy in Residential Aged Care: Mixed Methods Study
Abstract
Background: Apathy is a common symptom in neurological disorders, including dementia, and is associated with a faster rate of cognitive decline, reduced quality of life, and high caregiver burden. There is a lack of effective pharmacological treatments for apathy, and nonpharmacological interventions are a preferred first-line approach to treatment. Virtual reality (VR) using head-mounted displays (HMDs) is being successfully used in exposure- and distraction-based therapies; however, there is limited research on using HMDs for symptoms of neurological disorders.
Objective: This feasibility study aimed to assess whether VR using HMDs could be used to deliver tailored reminiscence therapy and examine the willingness to participate, response rates to measures, time taken to create tailored content, and technical problems. In addition, this study aimed to explore the immediate effects between verbal fluency and apathy after exposure to VR.
Methods: A mixed methods study was conducted in a sample of older adults residing in aged care, and 17 participants were recruited. Apathy was measured using the Apathy Evaluation Scale (AES), and verbal fluency was used as a proxy measure of improvements in apathy and debriefing interviews to assess feedback from participants. Side effects that can occur from using HMDs were also measured.
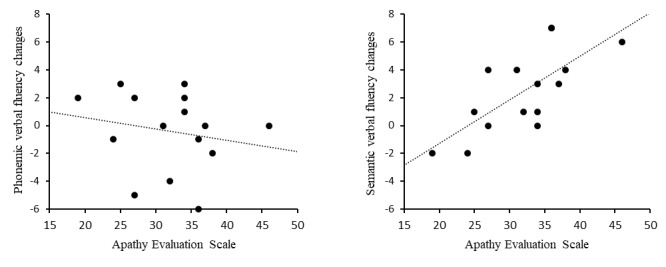
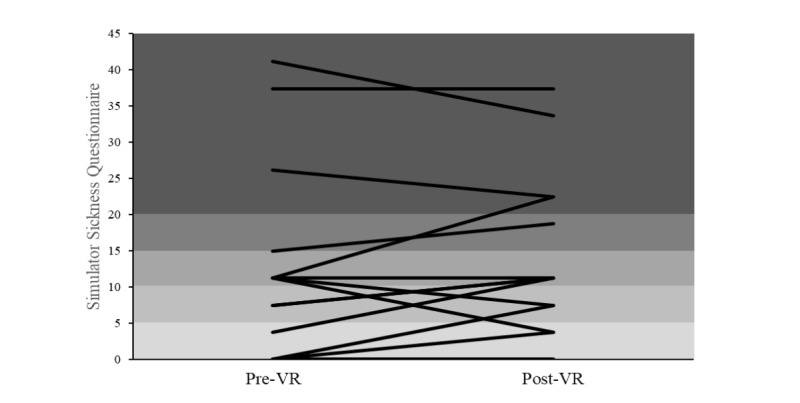
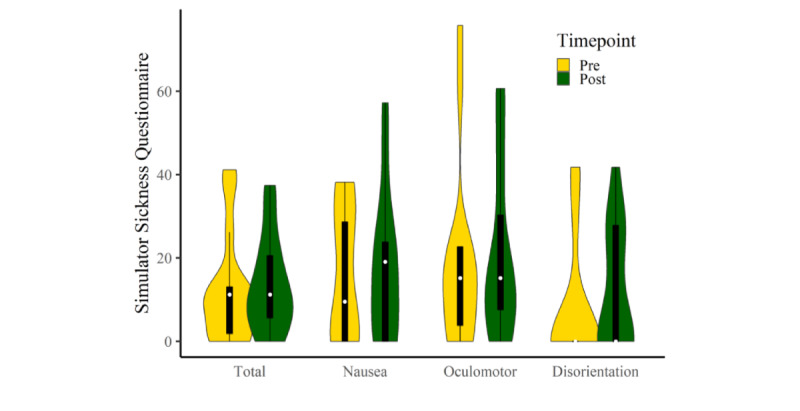
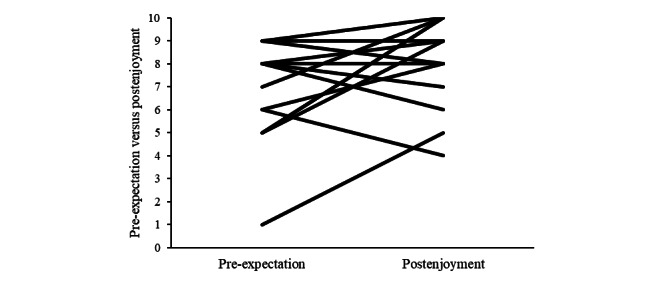
Results: We recruited participants from a high socioeconomic status setting with a high education level, and the participation rate was 85% (17/20); most responses to measures were positive. Access to a wide range of freely available content and the absence of technical difficulties made the delivery of a VR reminiscence intervention highly feasible. Participants had improved semantic scores (t14=-3.27; P=.006) but not phonemic fluency scores (t14=0.55; P=.59) immediately after the intervention. Those with higher levels of apathy demonstrated the greatest cognitive improvements after a VR reminiscence experience, which was indicated by a strong positive relationship between the AES and semantic verbal fluency change scores postminus pre-VR (r=0.719; 95% CI 0.327 to 0.900; P=.003). All participants enjoyed the experience despite 35% (6/17) of participants experiencing temporary side effects.
Conclusions: This study provides initial evidence that it is feasible to use VR with HMDs for therapy to treat symptoms of apathy in older adults in residential aged care. However, there is a need to closely monitor the side effects of HMD use in older adults. Further research is needed using an active control group to compare the use of VR with traditional forms of reminiscence therapy.
Keywords: apathy; cognitive aging; dementia; head-mounted display; reminiscence; residential facilities; virtual reality.
©Dimitrios Saredakis, Hannah AD Keage, Megan Corlis, Tobias Loetscher. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 26.06.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Virtual reality intervention to improve apathy in residential aged care: protocol for a multisite non-randomised controlled trial.BMJ Open. 2021 Feb 1;11(2):e046030. doi: 10.1136/bmjopen-2020-046030. BMJ Open. 2021. PMID: 33526504 Free PMC article. Clinical Trial.
-
The Effect of Reminiscence Therapy Using Virtual Reality on Apathy in Residential Aged Care: Multisite Nonrandomized Controlled Trial.J Med Internet Res. 2021 Sep 20;23(9):e29210. doi: 10.2196/29210. J Med Internet Res. 2021. PMID: 34542418 Free PMC article. Clinical Trial.
-
Preliminary Research: Virtual Reality in Residential Aged Care to Reduce Apathy and Improve Mood.Cyberpsychol Behav Soc Netw. 2020 Mar;23(3):165-170. doi: 10.1089/cyber.2019.0286. Epub 2019 Dec 12. Cyberpsychol Behav Soc Netw. 2020. PMID: 31829729
-
Augmented, Mixed, and Virtual Reality-Based Head-Mounted Devices for Medical Education: Systematic Review.JMIR Serious Games. 2021 Jul 8;9(3):e29080. doi: 10.2196/29080. JMIR Serious Games. 2021. PMID: 34255668 Free PMC article. Review.
-
Fully Immersive Virtual Reality Using 360° Videos to Manage Well-Being in Older Adults: A Scoping Review.J Am Med Dir Assoc. 2023 Apr;24(4):564-572. doi: 10.1016/j.jamda.2022.12.026. Epub 2023 Feb 6. J Am Med Dir Assoc. 2023. PMID: 36758621
Cited by
-
Veterans Affairs Health Care Provider Perceptions of Virtual Reality: Brief Exploratory Survey.Interact J Med Res. 2022 Sep 2;11(2):e38490. doi: 10.2196/38490. Interact J Med Res. 2022. PMID: 36053568 Free PMC article.
-
Ambient assisted living technology-mediated interventions for older people and their informal carers in the context of healthy ageing: A scoping review.Health Sci Rep. 2020 Dec 28;4(1):e225. doi: 10.1002/hsr2.225. eCollection 2021 Mar. Health Sci Rep. 2020. PMID: 33392394 Free PMC article.
-
Virtual reality intervention to improve apathy in residential aged care: protocol for a multisite non-randomised controlled trial.BMJ Open. 2021 Feb 1;11(2):e046030. doi: 10.1136/bmjopen-2020-046030. BMJ Open. 2021. PMID: 33526504 Free PMC article. Clinical Trial.
-
Exploring Virtual Reality-Based Reminiscence Therapy on Cognitive and Emotional Well-Being in People with Cognitive Impairments: A Scoping Review.Brain Sci. 2025 May 13;15(5):500. doi: 10.3390/brainsci15050500. Brain Sci. 2025. PMID: 40426671 Free PMC article. Review.
-
The Long-term Effects of Immersive Virtual Reality Reminiscence in People With Dementia: Longitudinal Observational Study.JMIR Serious Games. 2022 Jul 25;10(3):e36720. doi: 10.2196/36720. JMIR Serious Games. 2022. PMID: 35877169 Free PMC article.
References
-
- Skorvanek M, Rosenberger J, Gdovinova Z, Nagyova I, Saeedian RG, Groothoff JW, Dijk JP. Apathy in elderly nondemented patients with Parkinson's disease: clinical determinants and relationship to quality of life. J Geriatr Psychiatry Neurol. 2013 Dec;26(4):237–43. doi: 10.1177/0891988713500587. - DOI - PubMed
-
- Lanctôt KL, Agüera-Ortiz L, Brodaty H, Francis P, Geda Y, Ismail Z, Marshall GA, Mortby ME, Onyike CU, Padala PR, Politis AM, Rosenberg PB, Siegel E, Sultzer DL, Abraham EH. Apathy associated with neurocognitive disorders: recent progress and future directions. Alzheimers Dement. 2017 Jan;13(1):84–100. doi: 10.1016/j.jalz.2016.05.008. - DOI - PubMed
-
- Geda YE, Roberts RO, Mielke MM, Knopman DS, Christianson TJ, Pankratz VS, Boeve BF, Sochor O, Tangalos EG, Petersen RC, Rocca WA. Baseline neuropsychiatric symptoms and the risk of incident mild cognitive impairment: a population-based study. Am J Psychiatry. 2014 May;171(5):572–81. doi: 10.1176/appi.ajp.2014.13060821. http://europepmc.org/abstract/MED/24700290 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
