

Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review
- PMID: 32469387
- PMCID: PMC7484225
- DOI: 10.1001/jamaneurol.2020.2065
Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review
Abstract
Importance: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in December 2019, causing human coronavirus disease 2019 (COVID-19), which has now spread into a worldwide pandemic. The pulmonary manifestations of COVID-19 have been well described in the literature. Two similar human coronaviruses that cause Middle East respiratory syndrome (MERS-CoV) and severe acute respiratory syndrome (SARS-CoV-1) are known to cause disease in the central and peripheral nervous systems. Emerging evidence suggests COVID-19 has neurologic consequences as well.
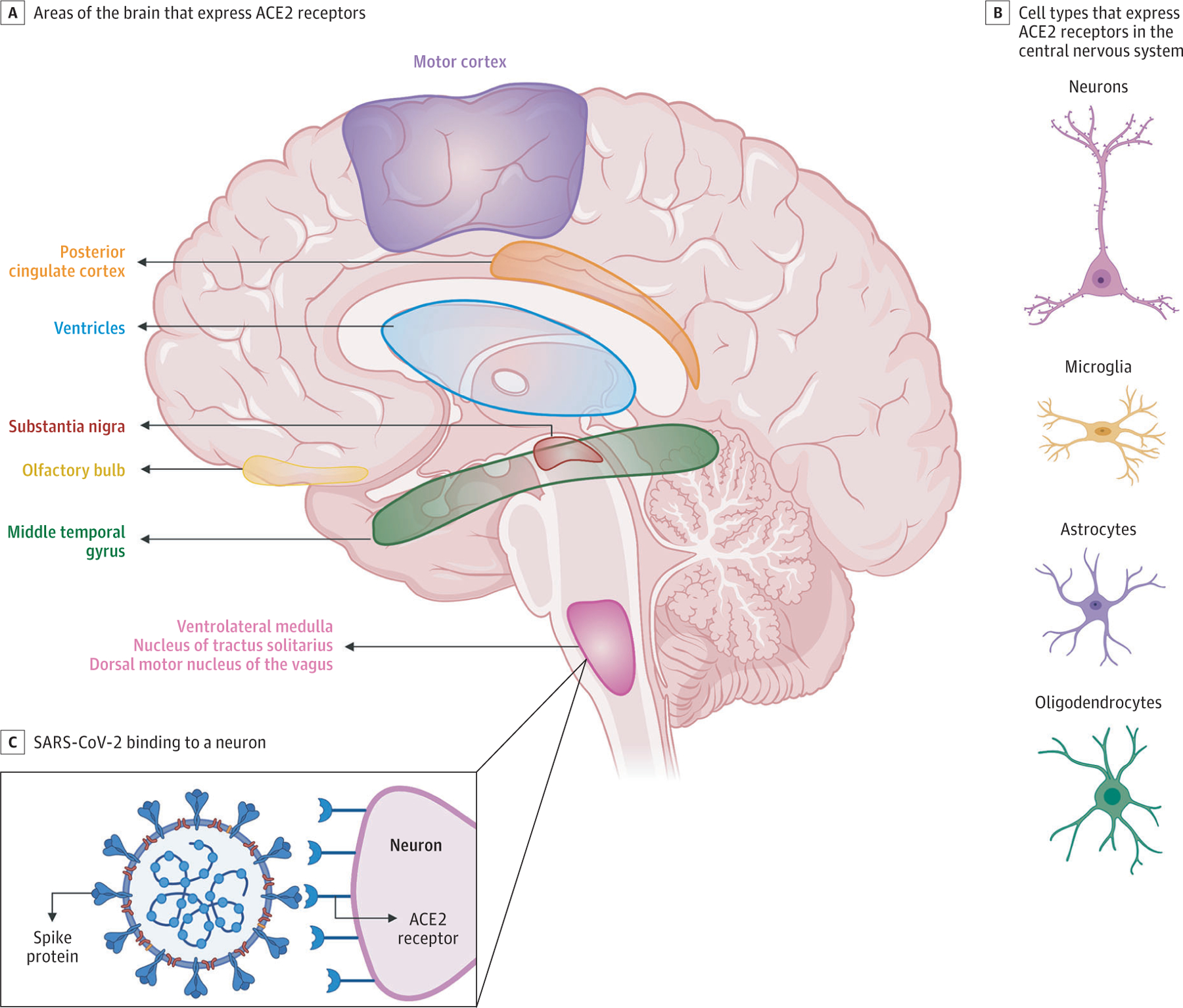
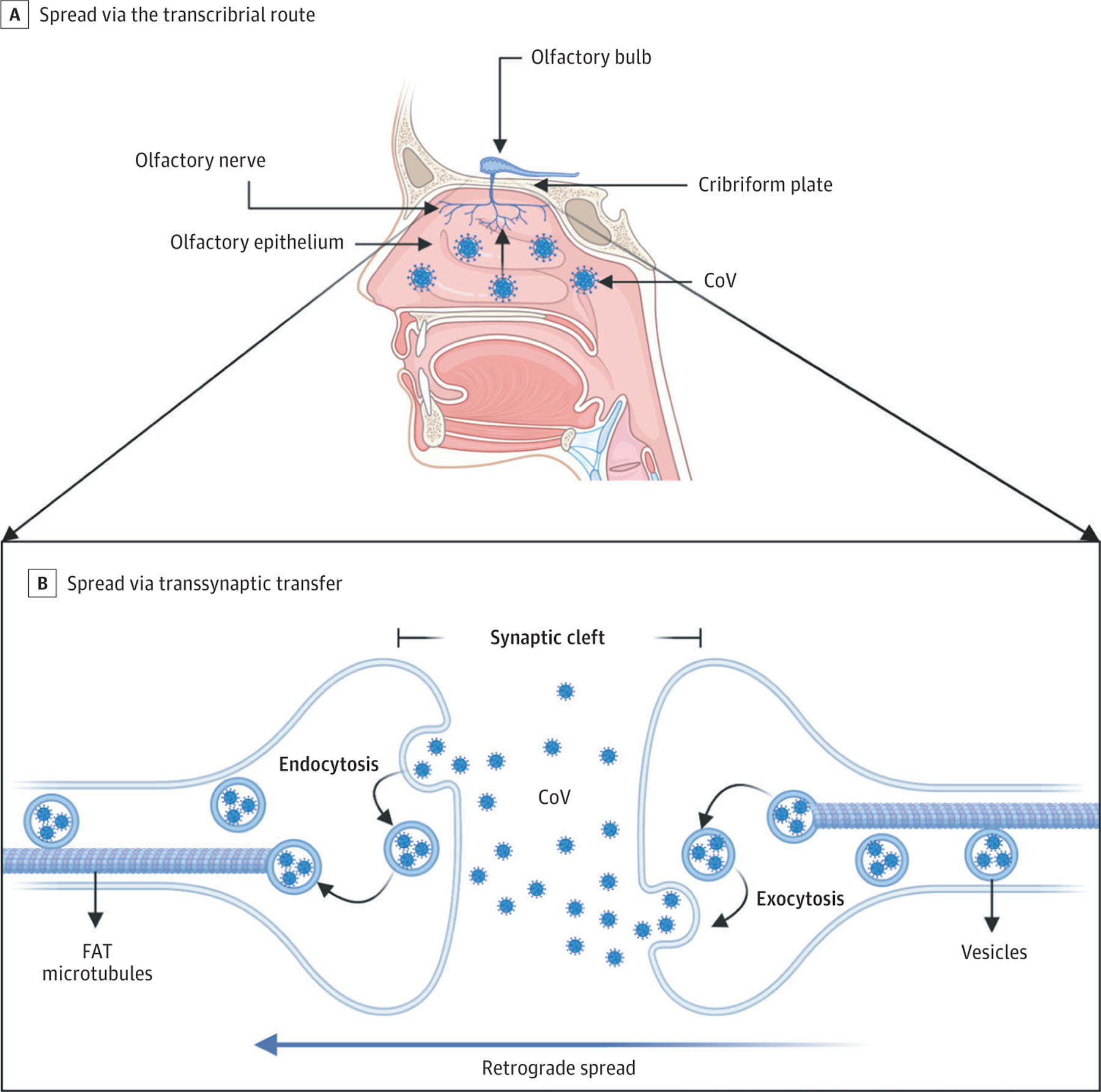
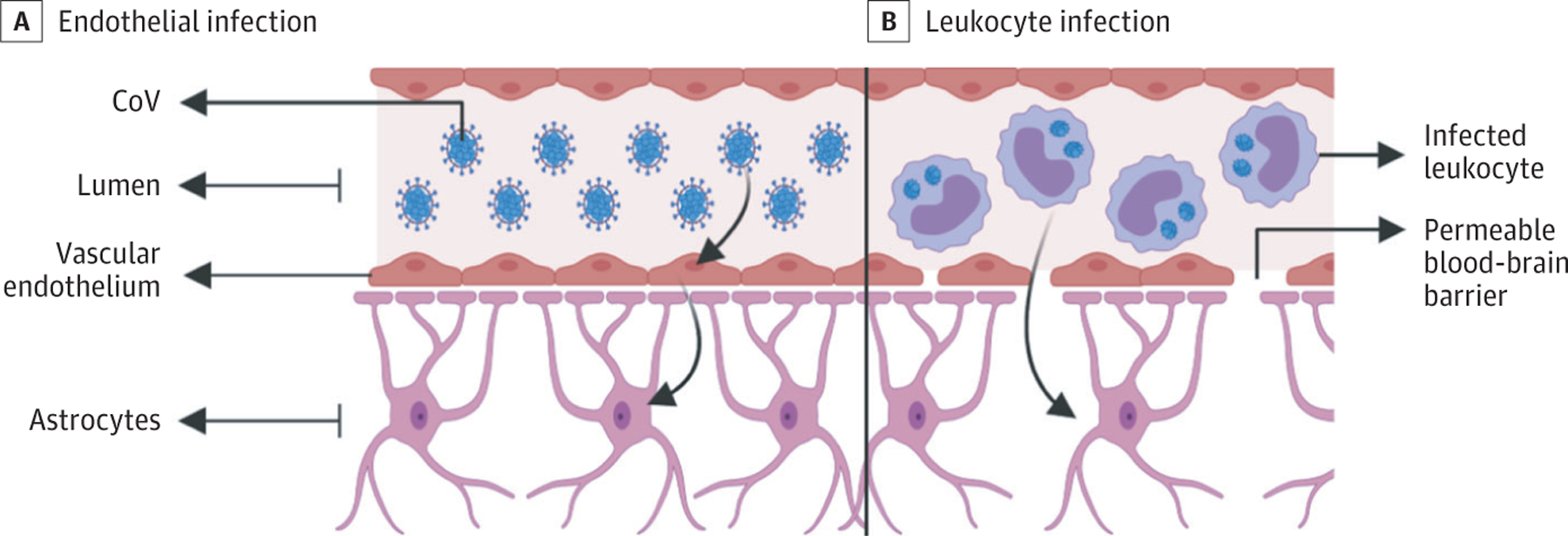
Observations: This review serves to summarize available information regarding coronaviruses in the nervous system, identify the potential tissue targets and routes of entry of SARS-CoV-2 into the central nervous system, and describe the range of clinical neurological complications that have been reported thus far in COVID-19 and their potential pathogenesis. Viral neuroinvasion may be achieved by several routes, including transsynaptic transfer across infected neurons, entry via the olfactory nerve, infection of vascular endothelium, or leukocyte migration across the blood-brain barrier. The most common neurologic complaints in COVID-19 are anosmia, ageusia, and headache, but other diseases, such as stroke, impairment of consciousness, seizure, and encephalopathy, have also been reported.
Conclusions and relevance: Recognition and understanding of the range of neurological disorders associated with COVID-19 may lead to improved clinical outcomes and better treatment algorithms. Further neuropathological studies will be crucial to understanding the pathogenesis of the disease in the central nervous system, and longitudinal neurologic and cognitive assessment of individuals after recovery from COVID-19 will be crucial to understand the natural history of COVID-19 in the central nervous system and monitor for any long-term neurologic sequelae.
Conflict of interest statement
Conflict of Interest Disclosures:
Dr Kuruvilla reported personal fees from Allergan, Lilly, Amgen, Theranica, and Now What Marketing outside the submitted work. Dr Spudich reported grants from National Institutes of Health (the National Institute of Mental Health and the National Institute of Neurological Disorders and Stroke) outside the submitted work. Dr Farhadian reports grant K23 MH118999 from the National Institute of Health (the National Institute of Mental Health) outside the submitted work. No other disclosures were reported.
Figures
Comment in
-
Letter to the Editor: New onset psychosis and mania following COVID-19 infection.J Psychiatr Res. 2020 Nov;130:177-179. doi: 10.1016/j.jpsychires.2020.07.042. Epub 2020 Aug 8. J Psychiatr Res. 2020. PMID: 32823051 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
