

Ramipril in High-Risk Patients With COVID-19
- PMID: 32470515
- PMCID: PMC7250557
- DOI: 10.1016/j.jacc.2020.05.040
Ramipril in High-Risk Patients With COVID-19
Abstract
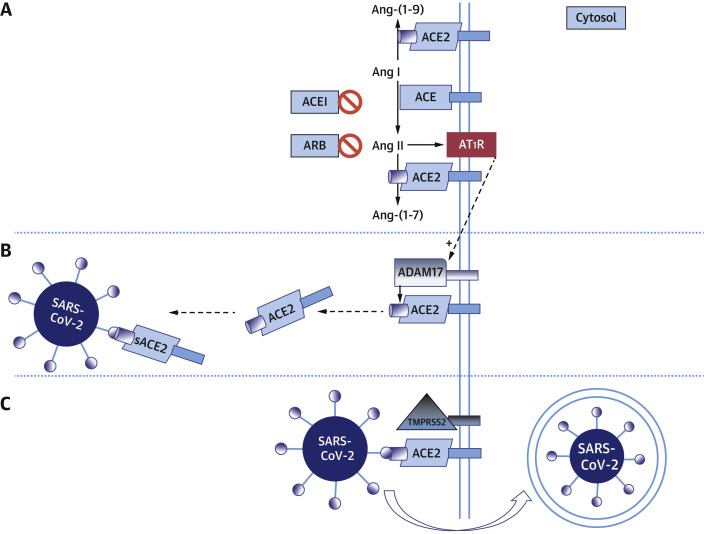
Background: Coronavirus disease-2019 (COVID-19) is caused by severe acute respiratory-syndrome coronavirus-2 that interfaces with the renin-angiotensin-aldosterone system (RAAS) through angiotensin-converting enzyme 2. This interaction has been proposed as a potential risk factor in patients treated with RAAS inhibitors.
Objectives: This study analyzed whether RAAS inhibitors modify the risk for COVID-19.
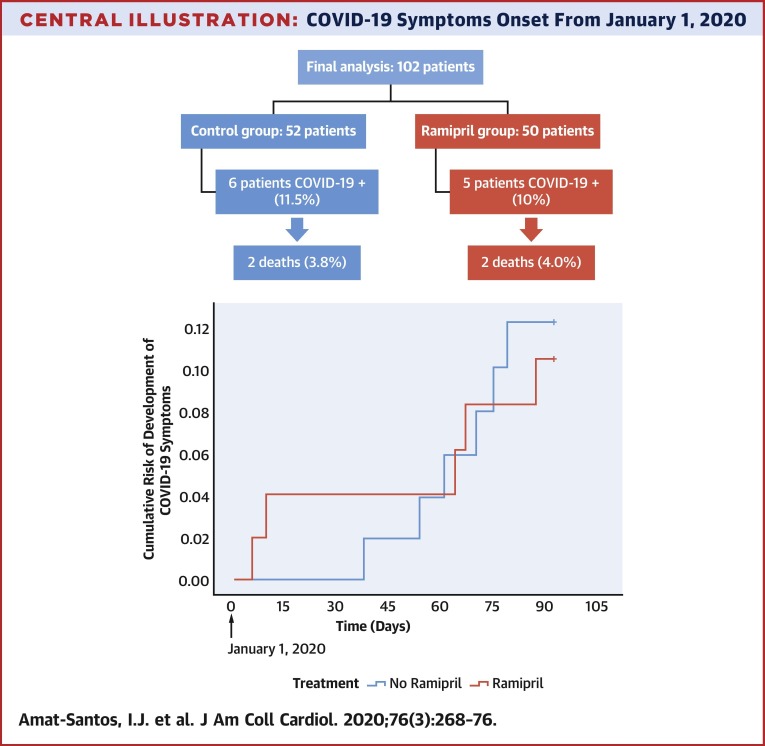
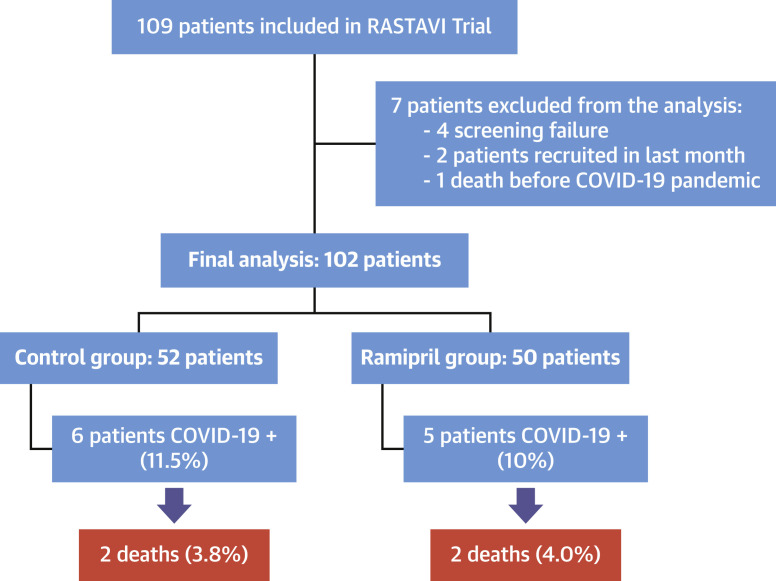
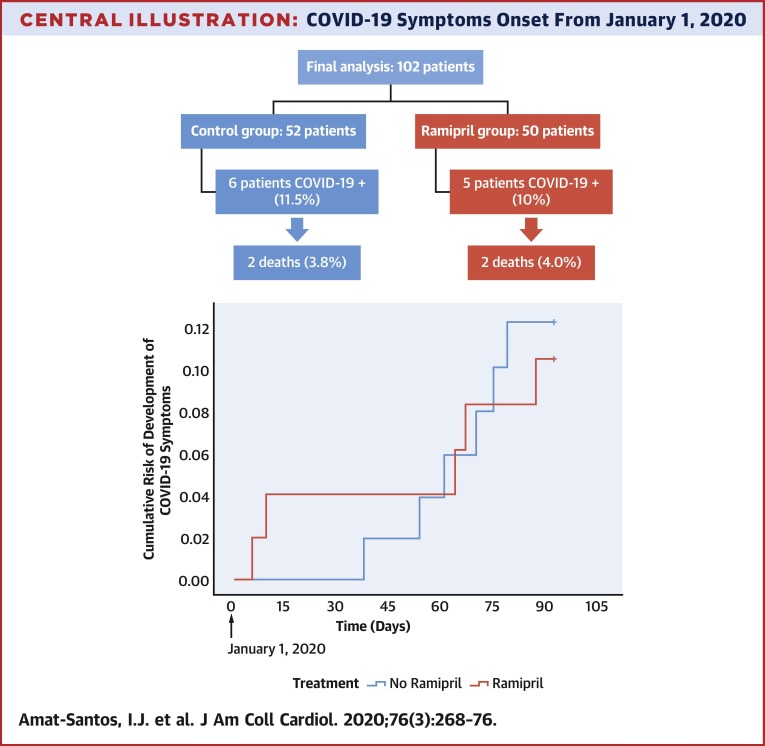
Methods: The RASTAVI (Renin-Angiotensin System Blockade Benefits in Clinical Evolution and Ventricular Remodeling After Transcatheter Aortic Valve Implantation) trial is an ongoing randomized clinical trial randomly allocating subjects to ramipril or control groups after successful transcatheter aortic valve replacement at 14 centers in Spain. A non-pre-specified interim analysis was performed to evaluate ramipril's impact on COVID-19 risk in this vulnerable population.
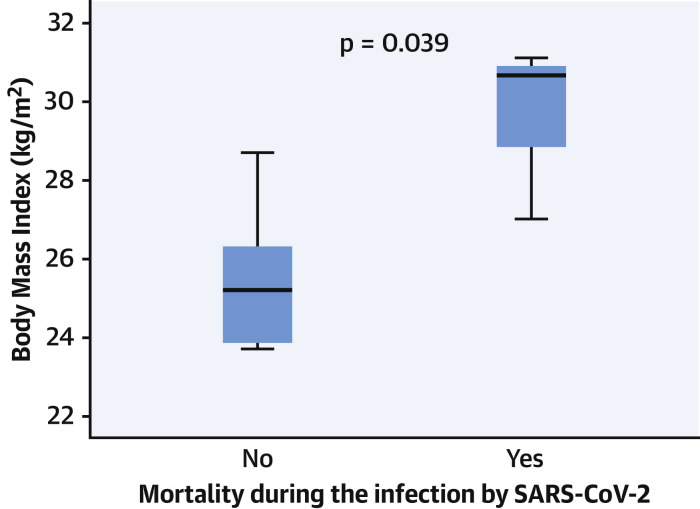
Results: As of April 1, 2020, 102 patients (50 in the ramipril group and 52 in the control group) were included in the trial. Mean age was 82.3 ± 6.1 years, 56.9% of the participants were male. Median time of ramipril treatment was 6 months (interquartile range: 2.9 to 11.4 months). Eleven patients (10.8%) have been diagnosed with COVID-19 (6 in control group and 5 receiving ramipril; hazard ratio: 1.150; 95% confidence interval: 0.351 to 3.768). The risk of COVID-19 was increased in older patients (p = 0.019) and those with atrial fibrillation (p = 0.066), lower hematocrit (p = 0.084), and more comorbidities according to Society of Thoracic Surgeons score (p = 0.065). Admission and oxygen supply was required in 4.9% of patients (2 in the ramipril group and 3 in the control group), and 4 of them died (2 in each randomized group). A higher body mass index was the only factor increasing the mortality rate (p = 0.039).
Conclusions: In a high-risk population of older patients with cardiovascular disease, randomization to ramipril had no impact on the incidence or severity of COVID-19. This analysis supports the maintenance of RAAS inhibitor treatment during the COVID-19 crisis. (Renin-Angiotensin System Blockade Benefits in Clinical Evolution and Ventricular Remodeling After Transcatheter Aortic Valve Implantation [RASTAVI]; NCT03201185).
Keywords: COVID-19; SARS-CoV-2; renin-angiotensin; transcatheter aortic valve replacement.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Renin-Angiotensin System Blockade in COVID-19: Good, Bad, or Indifferent?J Am Coll Cardiol. 2020 Jul 21;76(3):277-279. doi: 10.1016/j.jacc.2020.06.003. J Am Coll Cardiol. 2020. PMID: 32674791 Free PMC article.
-
ACE Inhibitors and Angiotensin II Receptor Blockers May Have Different Impact on Prognosis of COVID-19.J Am Coll Cardiol. 2020 Oct 27;76(17):2041. doi: 10.1016/j.jacc.2020.07.068. J Am Coll Cardiol. 2020. PMID: 33092742 Free PMC article. No abstract available.
References
-
- Drosten C., Günther S., Preiser W. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967–1976. - PubMed
-
- Zaki A.M., van Boheemen S., Bestebroer T.M., Osterhaus A.D., Fouchier R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–1820. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
