

Comparison between Diffusion-Weighted Sequences with Selective and Non-Selective Fat Suppression in the Evaluation of Crohn's Disease Activity: Are They Equally Useful?
- PMID: 32471191
- PMCID: PMC7345577
- DOI: 10.3390/diagnostics10060347
Comparison between Diffusion-Weighted Sequences with Selective and Non-Selective Fat Suppression in the Evaluation of Crohn's Disease Activity: Are They Equally Useful?
Abstract
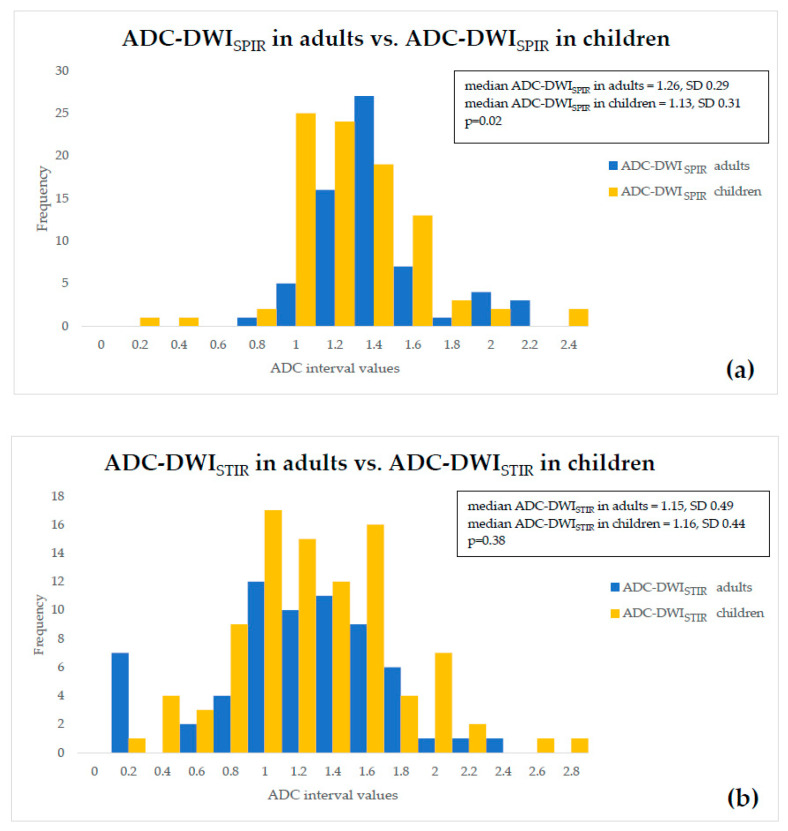
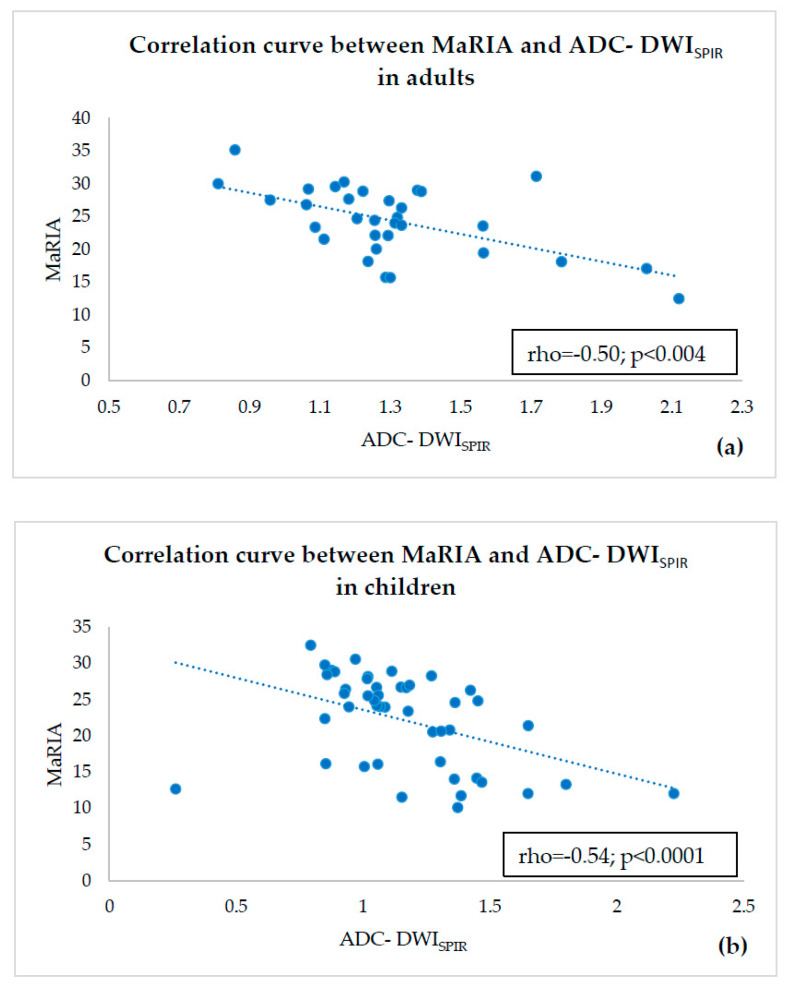
Background: We compared the efficiency of two MRI diffusion weighted imaging (DWI) techniques: DWI with SPIR (DWISPIR) and DWI with STIR (DWISTIR), to estimate their eligibility for quantitative assessment of Crohn's disease activity in children and adults. Methods: In inflamed terminal ileum segments (n = 32 in adults, n = 46 in children), Magnetic Resonance Index of Activity (MaRIA) was calculated, ADC values of both DWI techniques were measured, and the corresponding Clermont scores calculated. ADC values of both DWI techniques were compared between both and within each patient group, assessing their mutual correlation. Correlations between MaRIA and the corresponding ADC values, and Clermont scores based on both DWI techniques were estimated. Results: No correlation between ADC of DWISPIR and DWISTIR was observed (rho = 0.27, p = 0.13 in adults, rho = 0.20, p = 0.17 in children). The correlation between MaRIA and Clermont scores was strong in both techniques-in SPIR, rho = 0.93; p < 0.0005 in adults, rho = 0.98, p < 0.0005 in children, and, in STIR, rho = 0.89; p < 0.0005 in adults, rho = 0.95, p < 0.0005 in children. The correlation between ADC and MaRIA was moderate negative for DWISTIR (rho = 0.93, p < 0.0005 in adults, rho = 0.95, p < 0.0005 in children), but, in DWISTIR, no correlation between ADC and MaRIA score was observed in adults (rho = -0.001, p = 0.99), whereas children presented low negative correlation (rho = -0.374, p = 0.01). Conclusions: DWISTIR is not suitable for quantitative assessment of Crohn's disease activity both in children and adult patients.
Keywords: ADC; Clermont score; DWI; DWI fat suppression techniques.; DWIBS; MR enterography; MaRIA; diffusion-weighted imaging; terminal ileitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







Similar articles
-
Dynamic contrast-enhanced magnetic resonance imaging and diffusion-weighted imaging in the activity staging of terminal ileum Crohn's disease.World J Gastroenterol. 2020 Oct 21;26(39):6057-6073. doi: 10.3748/wjg.v26.i39.6057. World J Gastroenterol. 2020. PMID: 33132655 Free PMC article.
-
Evaluation of ileal Crohn's disease response to TNF antagonists: Validation of MR enterography for assessing response. Initial results.Eur J Radiol Open. 2020 Jan 28;7:100217. doi: 10.1016/j.ejro.2020.01.006. eCollection 2020. Eur J Radiol Open. 2020. PMID: 33102636 Free PMC article.
-
Diffusion-weighted imaging and apparent diffusion coefficient values for evaluating terminal ileitis in patients with Crohn's disease.Radiol Bras. 2019 Nov-Dec;52(6):361-367. doi: 10.1590/0100-3984.2019.0011. Radiol Bras. 2019. PMID: 32047329 Free PMC article.
-
Diffusion-weighted magnetic resonance imaging for detecting and assessing ileal inflammation in Crohn's disease.Aliment Pharmacol Ther. 2013 Mar;37(5):537-45. doi: 10.1111/apt.12201. Epub 2013 Jan 7. Aliment Pharmacol Ther. 2013. PMID: 23289713
-
Which MRI Score and Technique Should Be Used for Assessing Crohn's Disease Activity?J Clin Med. 2020 Jun 2;9(6):1691. doi: 10.3390/jcm9061691. J Clin Med. 2020. PMID: 32498279 Free PMC article. Review.
Cited by
-
Role of abbreviated non-contrast-enhanced MR-enterography in the evaluation of Crohn's disease activity and complications as an alternative for full protocol contrast-enhanced study: A systematic review and meta-analysis.Res Diagn Interv Imaging. 2023 Apr 28;6:100030. doi: 10.1016/j.redii.2023.100030. eCollection 2023 Jun. Res Diagn Interv Imaging. 2023. PMID: 39077544 Free PMC article.
References
-
- Dulai P.S., Singh S., Cesarini M., Bouguen G., Nelson S.A., Peyrin-Biroulet L., Feagan B.G., Ordas I., Sandborn W.J., Santillan C., et al. Cochrane Database of Systematic Reviews MRI scoring indices for evaluation of disease activity and severity in Crohn ’ s disease (Methodology Protocol) Cochrane Database Syst. Rev. 2015;4:1–8.
-
- Sakuraba H., Ishiguro Y., Hasui K., Hiraga H., Fukuda S., Shibutani K., Takai Y. Prediction of maintained mucosal healing in patients with Crohn’s disease under treatment with infliximab using diffusion-weighted magnetic resonance imaging. Digestion. 2014;89:49–54. doi: 10.1159/000356220. - DOI - PubMed
-
- Peyrin-Biroulet L., Sandborn W., Sands B.E., Reinisch W., Bemelman W., Bryant R.V., D’Haens G., Dotan I., Dubinsky M., Feagan B., et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am. J. Gastroenterol. 2015;110:1324–1338. doi: 10.1038/ajg.2015.233. - DOI - PubMed
-
- Maaser C., Sturm A., Vavricka S.R., Kucharzik T., Fiorino G., Annese V., Calabrese E., Baumgart D.C., Bettenworth D., Borralho Nunes P., et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn’s Colitis. 2019;13:144K–164K. doi: 10.1093/ecco-jcc/jjy113. - DOI - PubMed
LinkOut - more resources
Full Text Sources
