

Combined Coronary CT-Angiography and TAVI-Planning: A Contrast-Neutral Routine Approach for Ruling-out Significant Coronary Artery Disease
- PMID: 32471233
- PMCID: PMC7356559
- DOI: 10.3390/jcm9061623
Combined Coronary CT-Angiography and TAVI-Planning: A Contrast-Neutral Routine Approach for Ruling-out Significant Coronary Artery Disease
Abstract
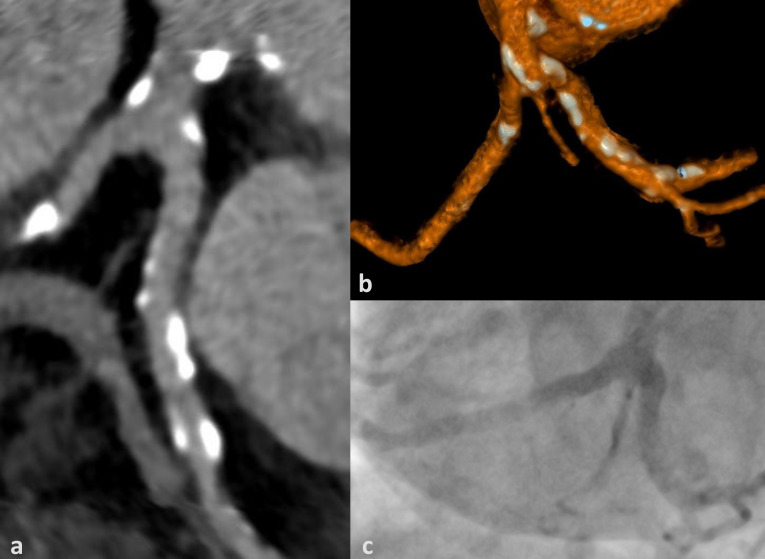
Background: Significant coronary artery disease (CAD) is a common finding in patients undergoing transcatheter aortic valve implantation (TAVI). Assessment of CAD prior to TAVI is recommended by current guidelines and is mainly performed via invasive coronary angiography (ICA). In this study we analyzed the ability of coronary CT-angiography (cCTA) to rule out significant CAD (stenosis ≥ 50%) during routine pre-TAVI evaluation in patients with high pre-test probability for CAD.
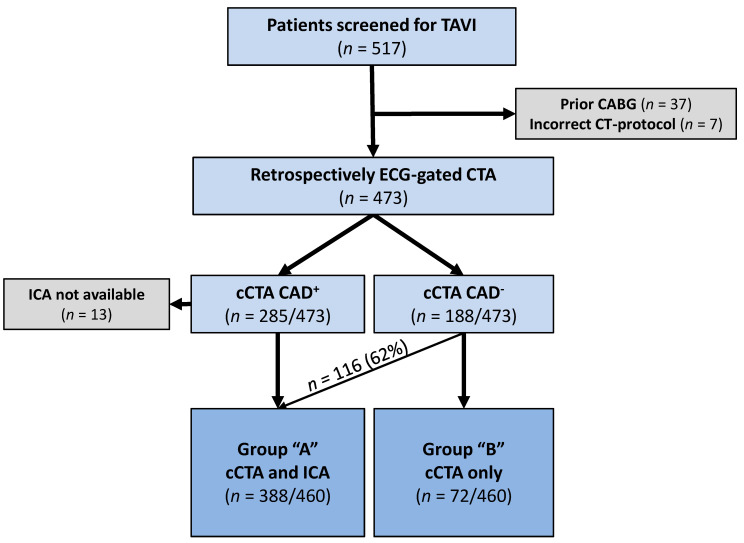
Methods: In total, 460 consecutive patients undergoing pre-TAVI CT (mean age 79.6 ± 7.4 years) were included. All patients were examined with a retrospectively ECG-gated CT-scan of the heart, followed by a high-pitch-scan of the vascular access route utilizing a single intravenous bolus of 70 ml iodinated contrast medium. Images were evaluated for image quality, calcifications, and significant CAD; CT-examinations in which CAD could not be ruled out were defined as positive (CAD+). Routinely, patients received ICA (388/460; 84.3%; Group A), which was omitted if renal function was impaired and CAD was ruled out on cCTA (Group B). Following TAVI, clinical events were documented during the hospital stay.
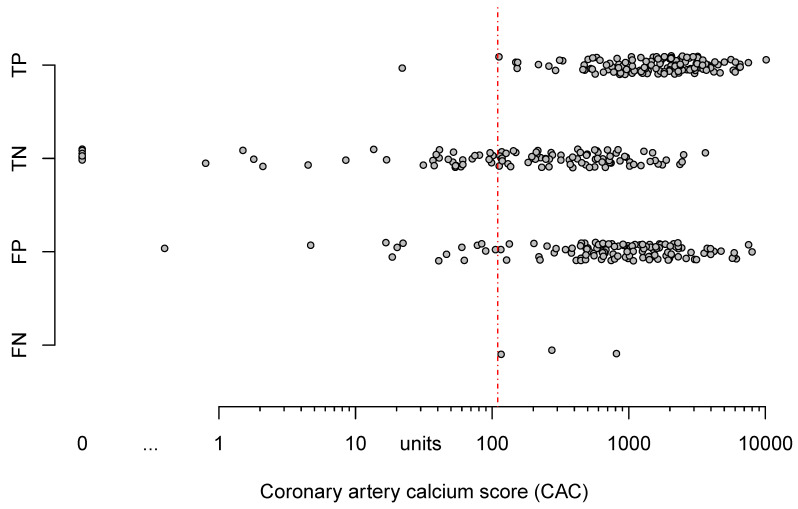
Results: cCTA was negative for CAD in 40.2% (188/460). Sensitivity, specificity, PPV, and NPV in Group A were 97.8%, 45.2%, 49.6%, and 97.4%, respectively. Median coronary artery calcium score (CAC) was higher in CAD+-patients but did not have predictive value for correct classification of patients with cCTA. There were no significant differences in clinical events between Group A and B.
Conclusion: cCTA can be incorporated into pre-TAVI CT-evaluation with no need for additional contrast medium. cCTA may exclude significant CAD in a relatively high percentage of these high-risk patients. Thereby, cCTA may have the potential to reduce the need for ICA and total amount of contrast medium applied, possibly making pre-procedural evaluation for TAVI safer and faster.
Keywords: aortic stenosis; computed tomography coronary angiography; coronary angiography; coronary artery disease; diagnostic accuracy; transcatheter aortic valve implantation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Nishimura R.A., Otto C.M., Bonow R.O., Carabello B.A., Erwin J.P., Fleisher L.A., Jneid H., Mack M.J., McLeod C.J., O’Gara P.T., et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2017;70:252–289. doi: 10.1016/j.jacc.2017.03.011. - DOI - PubMed
-
- Mack M.J., Leon M.B., Thourani V.H., Makkar R., Kodali S.K., Russo M., Kapadia S.R., Malaisrie S.C., Cohen D.J., Pibarot P., et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019;380:1695–1705. doi: 10.1056/NEJMoa1814052. - DOI - PubMed
-
- Blanke P., Weir-McCall J.R., Achenbach S., Delgado V., Hausleiter J., Jilaihawi H., Marwan M., Nørgaard B.L., Piazza N., Schoenhagen P., et al. Computed Tomography Imaging in the Context of Transcatheter Aortic Valve Implantation (TAVI)/Transcatheter Aortic Valve Replacement (TAVR): An Expert Consensus Document of the Society of Cardiovascular Computed Tomography. JACC Cardiovasc. Imaging. 2019;12:1–24. doi: 10.1016/j.jcmg.2018.12.003. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
