

Validation of Pharmacological Protocols for Targeted Inhibition of Canalicular MRP2 Activity in Hepatocytes Using [99mTc]mebrofenin Imaging in Rats
- PMID: 32471244
- PMCID: PMC7355955
- DOI: 10.3390/pharmaceutics12060486
Validation of Pharmacological Protocols for Targeted Inhibition of Canalicular MRP2 Activity in Hepatocytes Using [99mTc]mebrofenin Imaging in Rats
Abstract
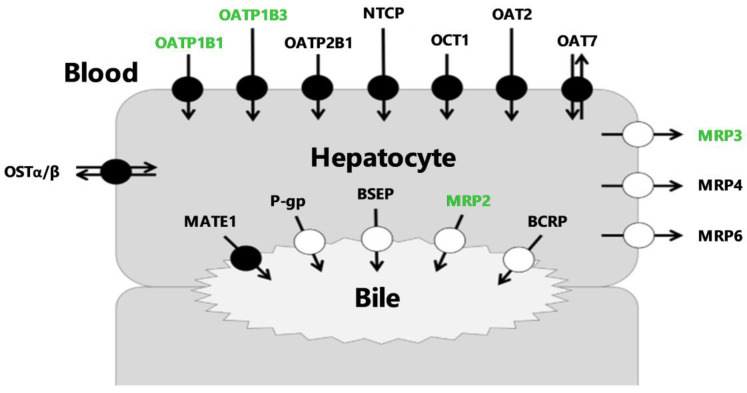
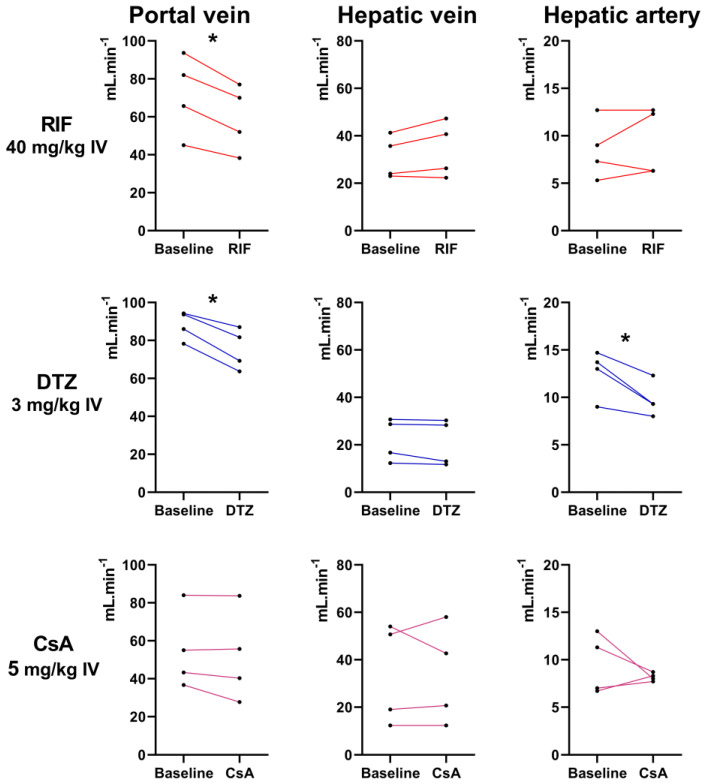
The multidrug resistance-associated protein 2 (MRP2) mediates the biliary excretion of drugs and metabolites. [99mTc]mebrofenin may be employed as a probe for hepatic MRP2 activity because its biliary excretion is predominantly mediated by this transporter. As the liver uptake of [99mTc]mebrofenin depends on organic anion-transporting polypeptide (OATP) activity, a safe protocol for targeted inhibition of hepatic MRP2 is needed to study the intrinsic role of each transporter system. Diltiazem (DTZ) and cyclosporin A (CsA) were first confirmed to be potent MRP2 inhibitors in vitro. Dynamic acquisitions were performed in rats (n = 5-6 per group) to assess the kinetics of [99mTc]mebrofenin in the liver, intestine and heart-blood pool after increasing doses of inhibitors. Their impact on hepatic blood flow was assessed using Doppler ultrasound (n = 4). DTZ (s.c., 10 mg/kg) and low-dose CsA (i.v., 0.01 mg/kg) selectively decreased the transfer of [99mTc]mebrofenin from the liver to the bile (k3). Higher doses of DTZ and CsA did not further decrease k3 but dose-dependently decreased the uptake (k1) and backflux (k2) rate constants between blood and liver. High dose of DTZ (i.v., 3 mg/kg) but not CsA (i.v., 5 mg/kg) significantly decreased the blood flow in the portal vein and hepatic artery. Targeted pharmacological inhibition of hepatic MRP2 activity can be achieved in vivo without impacting OATP activity and liver blood flow. Clinical studies are warranted to validate [99mTc]mebrofenin in combination with low-dose CsA as a novel substrate/inhibitor pair to untangle the role of OATP and MRP2 activity in liver diseases.
Keywords: drug metabolism; drug-induced liver injury; imaging; liver; membrane transporter; pharmacokinetics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Evers R., Piquette-Miller M., Polli J., Russel F., Sprowl J.A., Tohyama K., Ware J., de Wildt S., Xie W., Brouwer K. Disease-associated changes in drug transporters may impact the pharmacokinetics and/or toxicity of drugs: A white paper from the international transporter consortium. Clin. Pharmacol. Ther. 2018;104:900–915. doi: 10.1002/cpt.1115. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
