

Severe HELLP syndrome masquerading as thrombocytopenic thrombotic purpura: a case report
- PMID: 32471388
- PMCID: PMC7260815
- DOI: 10.1186/s12882-020-01865-y
Severe HELLP syndrome masquerading as thrombocytopenic thrombotic purpura: a case report
Abstract
Background: Thrombotic microangiopathies (TMAs) occurring in the postpartum period may be difficult to manage. They present as the combination of mechanical hemolytic anemia and consumption thrombocytopenia due to endothelial dysfunction. The cause of this endothelial aggression can be multiple: thrombocytopenic thrombotic purpura (TTP), HELLP syndrome, antiphospholipid syndrome, atypical hemolytic and uremic syndrome or acute fatty liver of pregnancy. TTP results from a severe deficiency of ADAMTS13, which is a protease cleaving specifically von Willebrand factor chiefly produced by liver cells. There are two main causes, the production of anti-ADAMTS13 auto-antibodies and, more rarely, a genetic deficiency in ADAMTS13. First-line treatment is based on plasma exchange. HELLP syndrome occurs in the third trimester of pregnancy usually in association with preeclampsia and represents a form of TMA characterized by damage to the sinusoidal capillaries of the liver. Prompt delivery is the main treatment. We present a case illustrating the challenges in discriminating between different postpartum TMAs, with a focus on the distinction between TTP and HELLP syndrome. Specifically, we highlight how acute liver failure (ALF) stemming from HELLP may lead to TTP with a spectacular response to plasma exchanges.
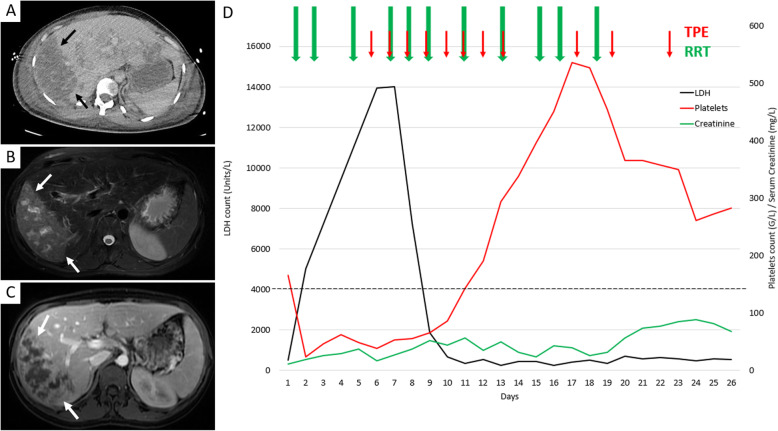
Case: A 28-year-old, 33 + 4 weeks pregnant woman presented with severe preeclampsia complicated by ALF in the setting of partial liver necrosis, disseminated intravascular coagulation, microangiopathic hemolytic anemia and acute kidney injury. Greatly diminished levels of ADAMTS13 (< 5%) activity and neurological impairment suggested an initial diagnosis of thrombotic thrombocytopenic purpura (TTP). Therapeutic plasma exchange (TPE) was initiated and complete renal, neurological, hematological and hepatic recovery was observed. Secondary TTP induced by ALF due to HELLP syndrome was the final diagnosis.
Conclusion: Our case addresses the overlapping nature of postpartum TMAs and raises the possibility that HELLP-induced ALF may constitute an additional mechanism resulting in TTP, thereby opening a possible indication for TPE.
Keywords: Acute liver failure; Case report; HELLP syndrome; Therapeutic plasma exchange; Thrombotic microangiopathy; Thrombotic thrombocytopenic purpura.
Conflict of interest statement
AH is an Editorial Board Member of BMC Nephrology.
Figures
References
-
- Joly BS, Coppo P, Veyradier A. Thrombotic thrombocytopenic purpura. Blood. 2017;129(21):2836–2846. - PubMed
-
- Scully M, Thomas M, Underwood M, Watson H, Langley K, Camilleri RS, et al. Thrombotic thrombocytopenic purpura and pregnancy: presentation, management, and subsequent pregnancy outcomes. Blood. 2014;124(2):211–219. - PubMed
-
- Wallace K, Martin JN, Tam Tam K, Wallukat G, Dechend R, Lamarca B, et al. Seeking the mechanism(s) of action for corticosteroids in HELLP syndrome: SMASH study. Am J Obstet Gynecol. 2013;208(5):380.e1–380.e8. - PubMed
-
- Moatti-Cohen M, Garrec C, Wolf M, Boisseau P, Galicier L, Azoulay E, et al. Unexpected frequency of Upshaw-Schulman syndrome in pregnancy-onset thrombotic thrombocytopenic purpura. Blood. 2012;119(24):5888–5897. - PubMed
-
- Yoshihara M, Mayama M, Ukai M, Tano S, Kishigami Y, Oguchi H. Fulminant liver failure resulting from massive hepatic infarction associated with hemolysis, elevated liver enzymes, and low platelets syndrome. J Obstet Gynaecol Res. 2016;42(10):1375–1378. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
