

Risk factors and the natural history of accelerated knee osteoarthritis: a narrative review
- PMID: 32471412
- PMCID: PMC7260785
- DOI: 10.1186/s12891-020-03367-2
Risk factors and the natural history of accelerated knee osteoarthritis: a narrative review
Abstract
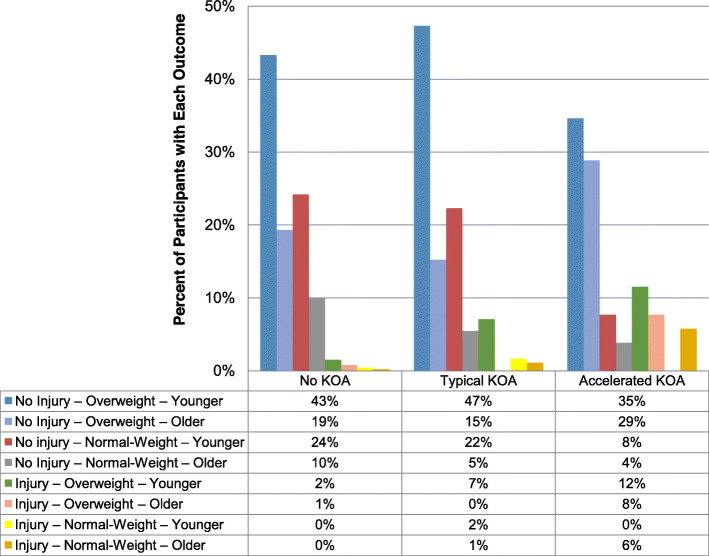
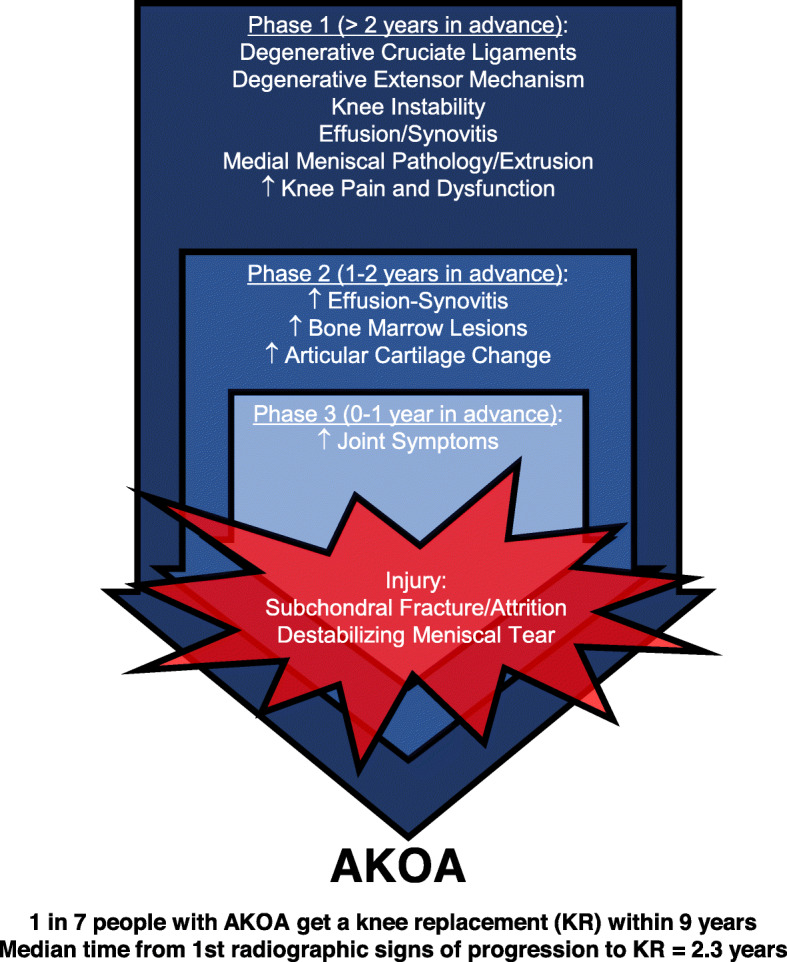
Background: Osteoarthritis is generally a slowly progressive disorder. However, at least 1 in 7 people with incident knee osteoarthritis develop an abrupt progression to advanced-stage radiographic disease, many within 12 months. We summarize what is known - primarily based on findings from the Osteoarthritis Initiative - about the risk factors and natural history of accelerated knee osteoarthritis (AKOA) - defined as a transition from no radiographic knee osteoarthritis to advanced-stage disease < 4 years - and put these findings in context with typical osteoarthritis (slowly progressing disease), aging, prior case reports/series, and relevant animal models. Risk factors in the 2 to 4 years before radiographic manifestation of AKOA (onset) include older age, higher body mass index, altered joint alignment, contralateral osteoarthritis, greater pre-radiographic disease burden (structural, symptoms, and function), or low fasting glucose. One to 2 years before AKOA onset people often exhibit rapid articular cartilage loss, larger bone marrow lesions and effusion-synovitis, more meniscal pathology, slower chair-stand or walking pace, and increased global impact of arthritis than adults with typical knee osteoarthritis. Increased joint symptoms predispose a person to new joint trauma, which for someone who develops AKOA is often characterized by a destabilizing meniscal tear (e.g., radial or root tear). One in 7 people with AKOA onset subsequently receive a knee replacement during a 9-year period. The median time from any increase in radiographic severity to knee replacement is only 2.3 years. Despite some similarities, AKOA is different than other rapidly progressive arthropathies and collapsing these phenomena together or extracting results from one type of osteoarthritis to another should be avoided until further research comparing these types of osteoarthritis is conducted. Animal models that induce meniscal damage in the presence of other risk factors or create an incongruent distribution of loading on joints create an accelerated form of osteoarthritis compared to other models and may offer insights into AKOA.
Conclusion: Accelerated knee osteoarthritis is unique from typical knee osteoarthritis. The incidence of AKOA in the Osteoarthritis Initiative and Chingford Study is substantial. AKOA needs to be taken into account and studied in epidemiologic studies and clinical trials.
Keywords: Knee; Magnetic resonance imaging; Meniscus; Natural history; Osteoarthritis; Phenotype; Radiography; Risk factors.
Conflict of interest statement
JBD, MFB, and MSH are members of the Editorial Board of BMC Musculoskeletal Disorders. JBD also reported payment for lectures from Pfizer, Inc. and consultancy from Pfizer/Lilly. TEM reported consultancy from Pfizer, Sanofi Aventis US, Kolon Tissuegene, Samumed, Seikagaku, Kiniksa Pharmaceuticals, and Anika Therapeutics. The other authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
