

Interplay of somatic alterations and immune infiltration modulates response to PD-1 blockade in advanced clear cell renal cell carcinoma
- PMID: 32472114
- PMCID: PMC7499153
- DOI: 10.1038/s41591-020-0839-y
Interplay of somatic alterations and immune infiltration modulates response to PD-1 blockade in advanced clear cell renal cell carcinoma
Abstract
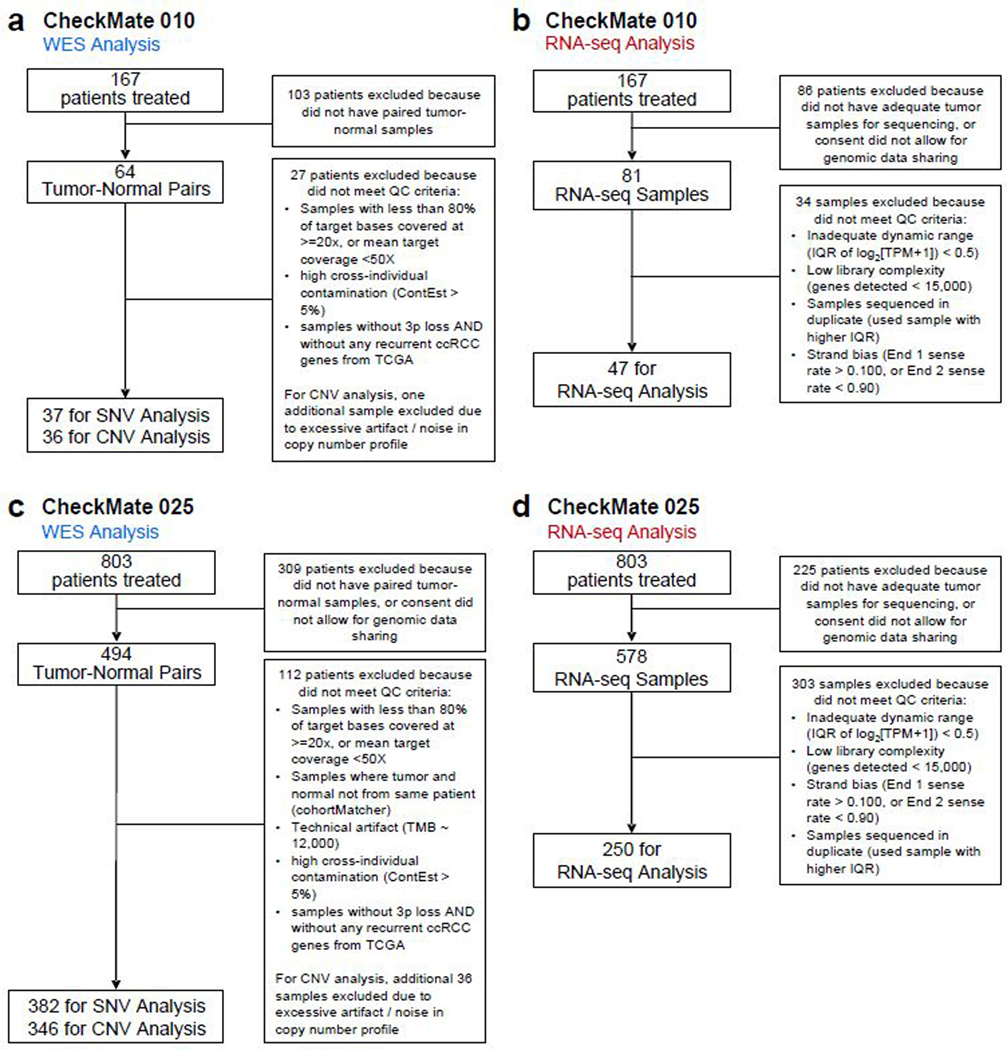
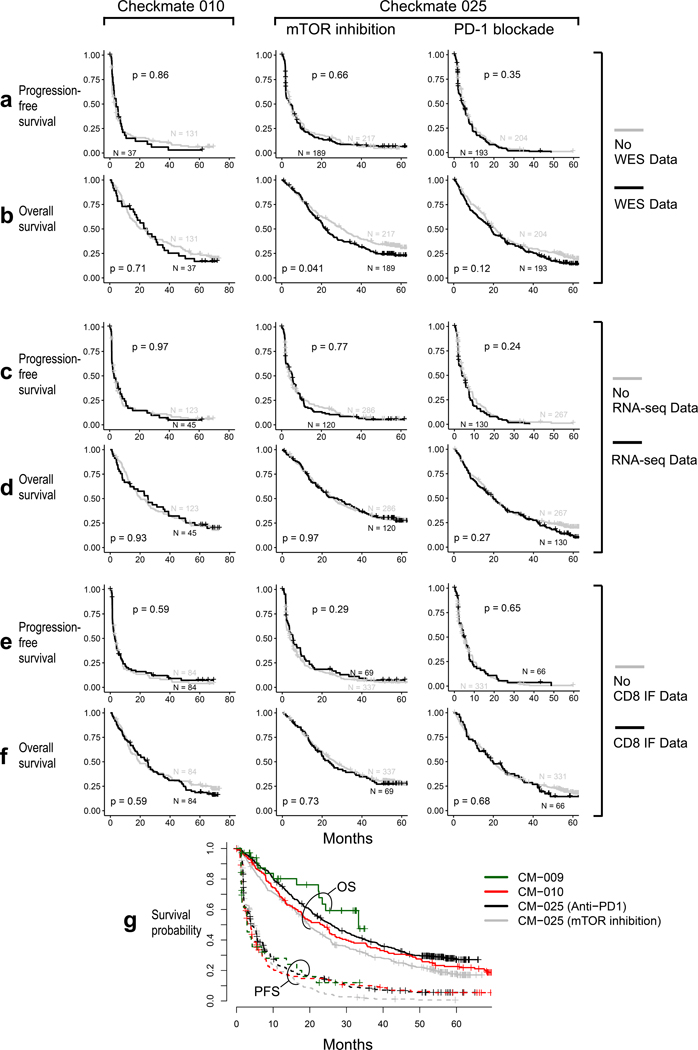
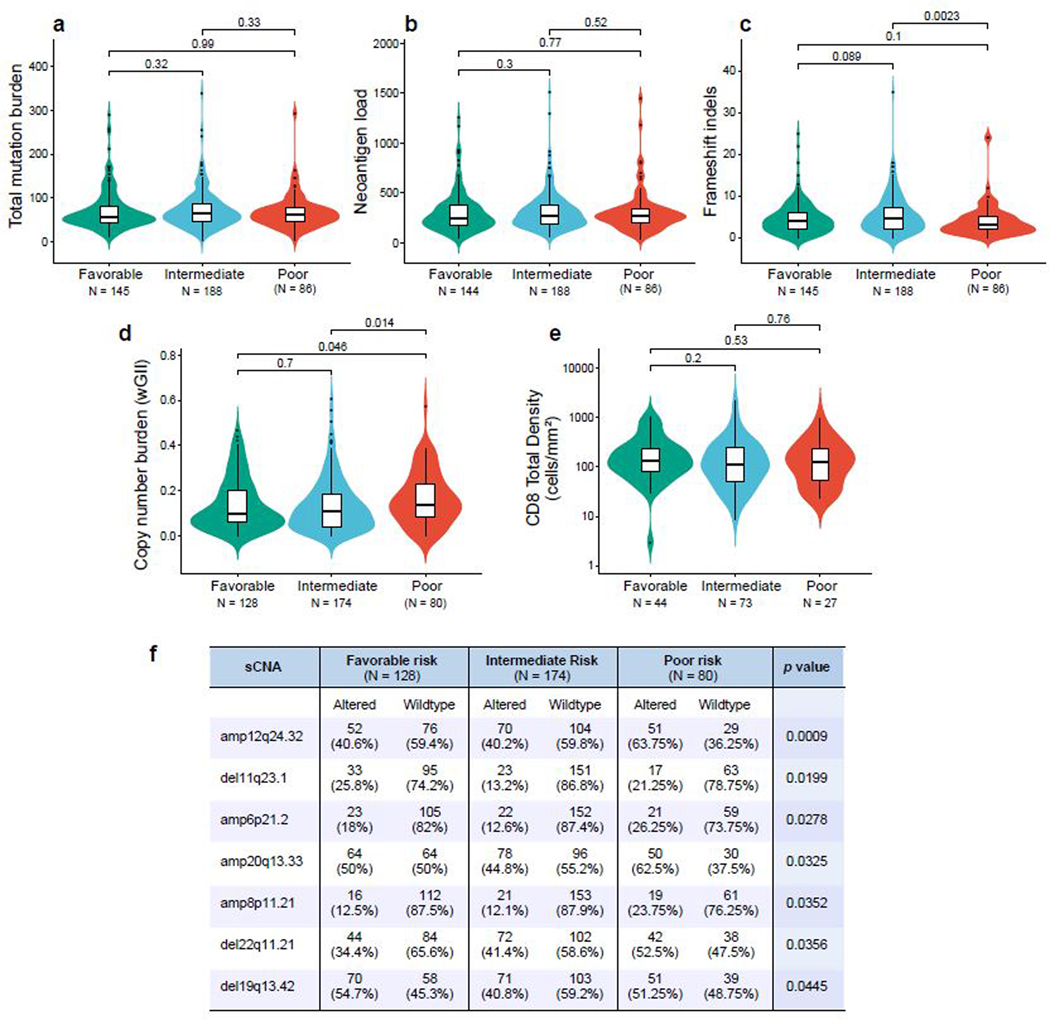
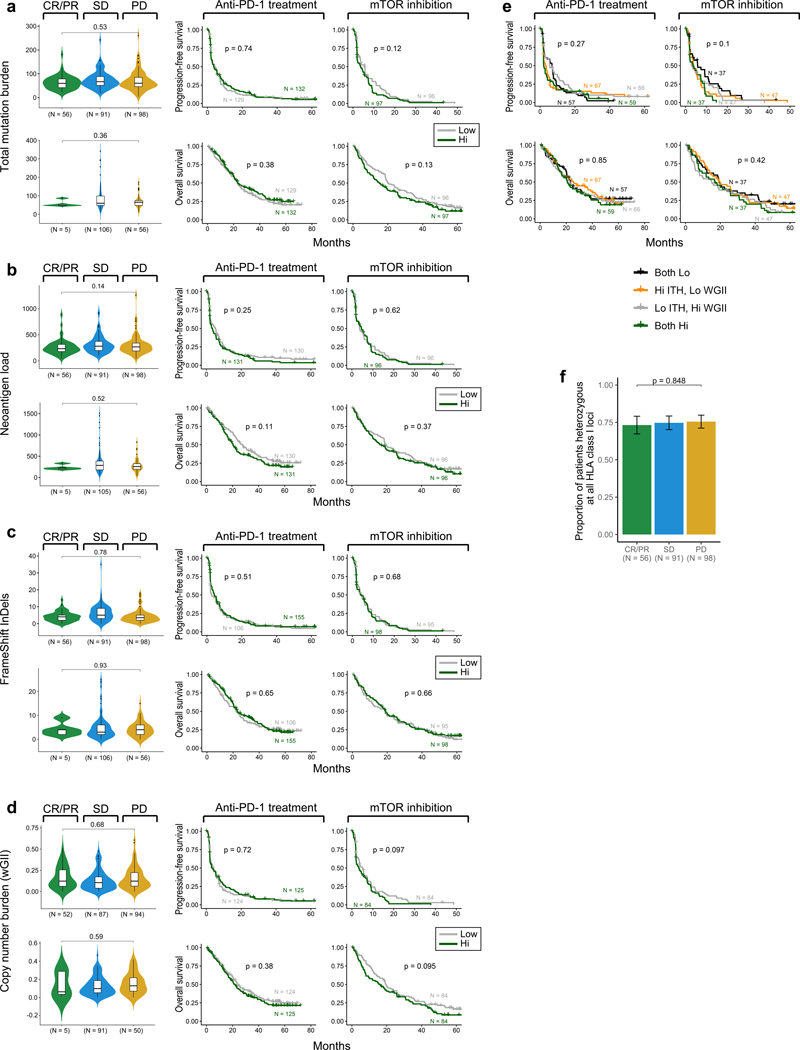
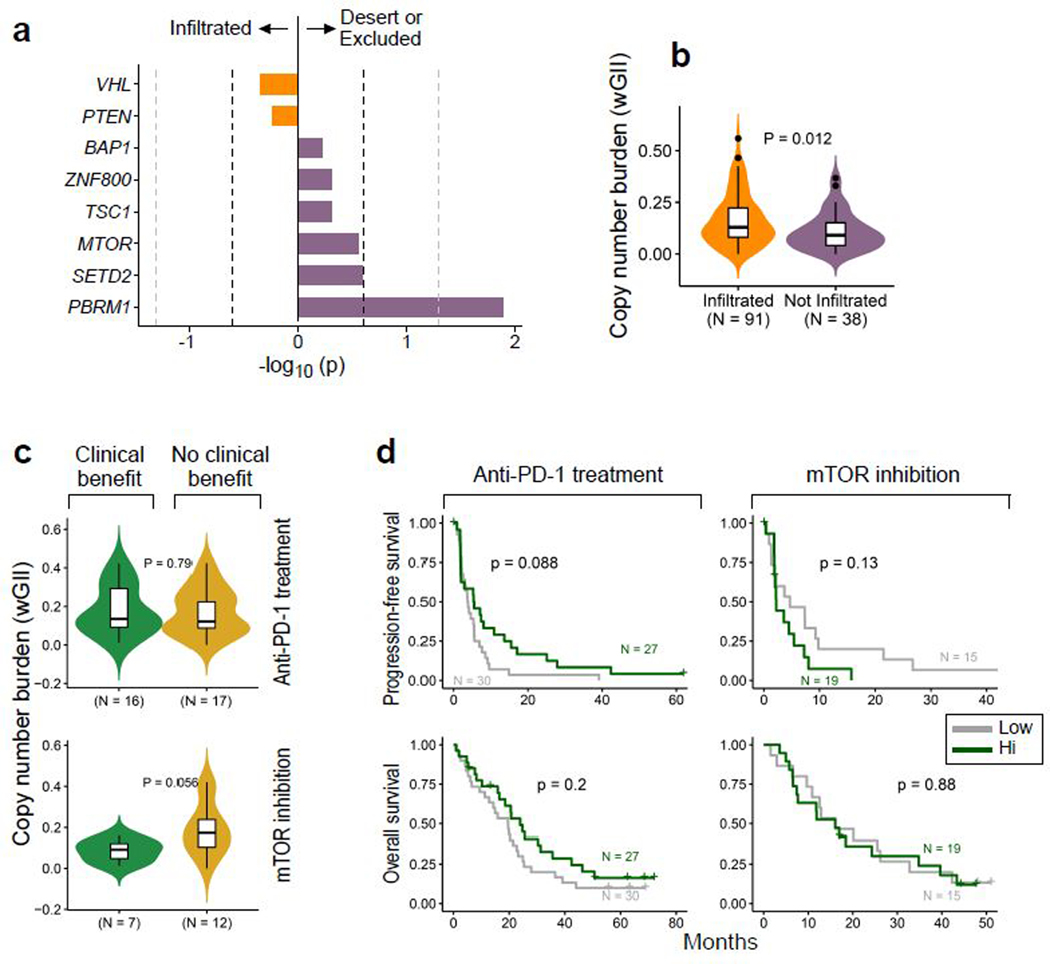
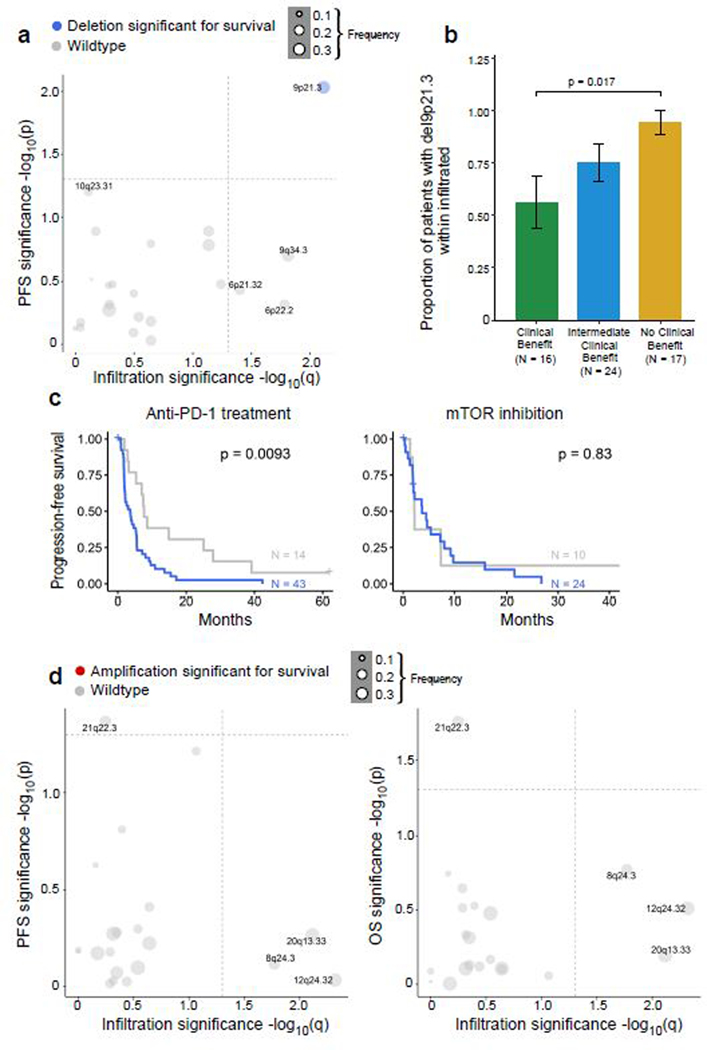
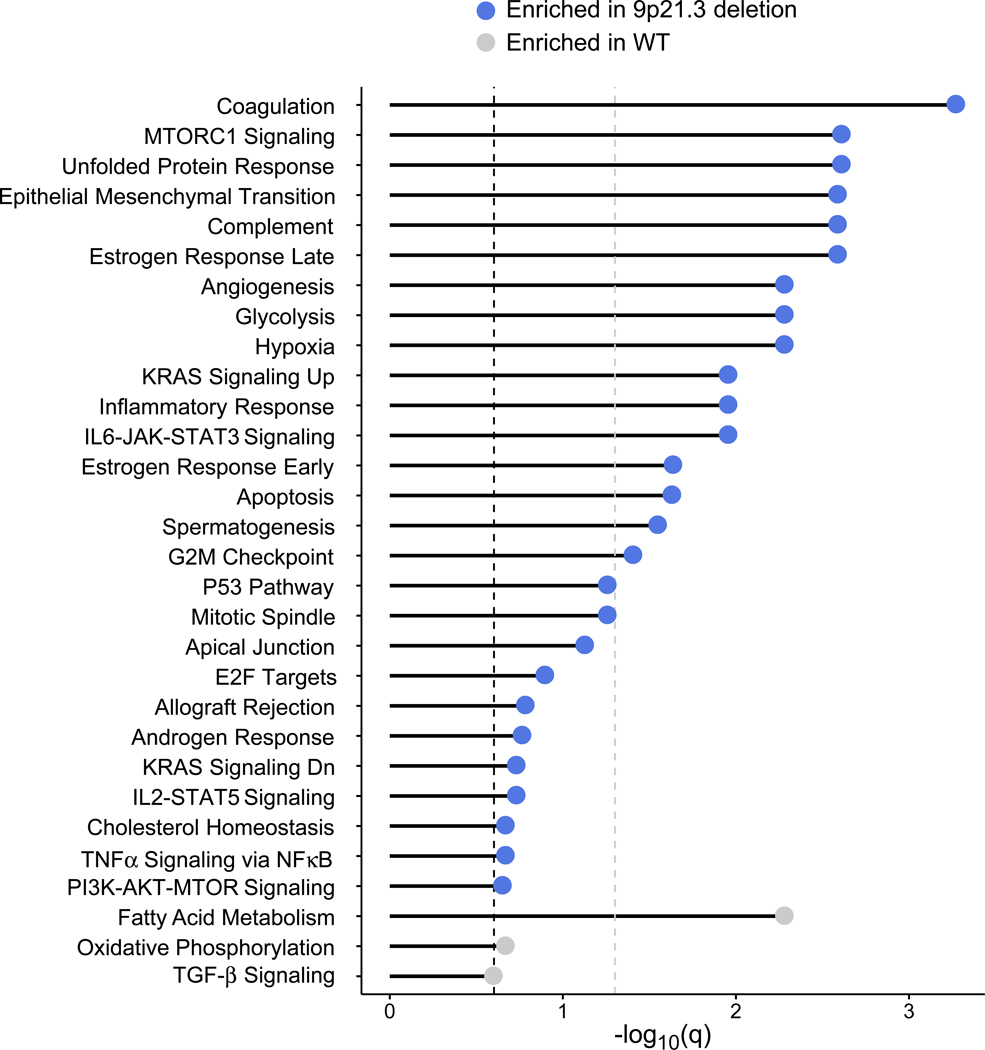
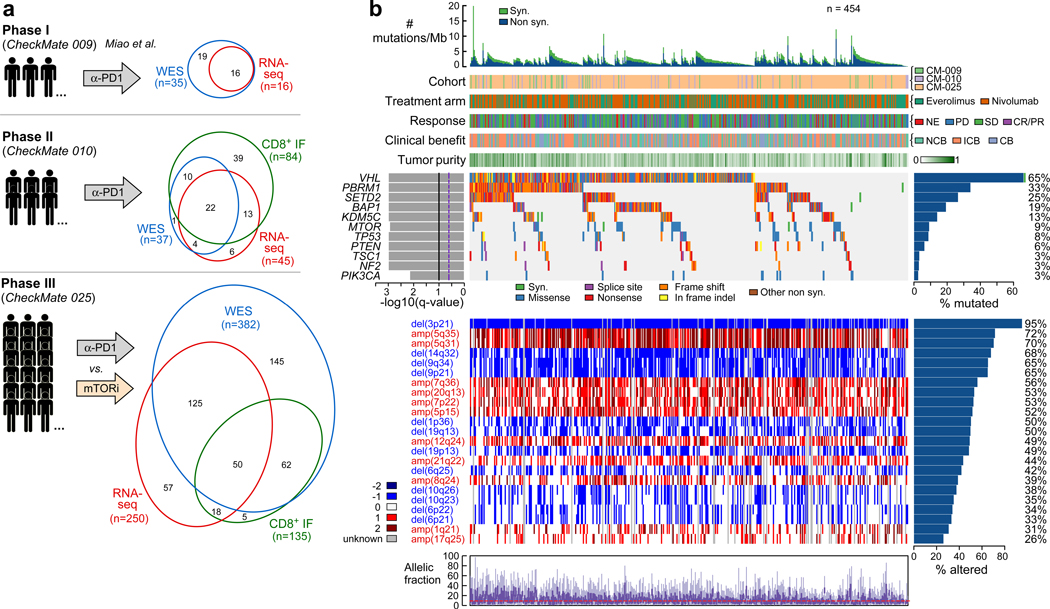
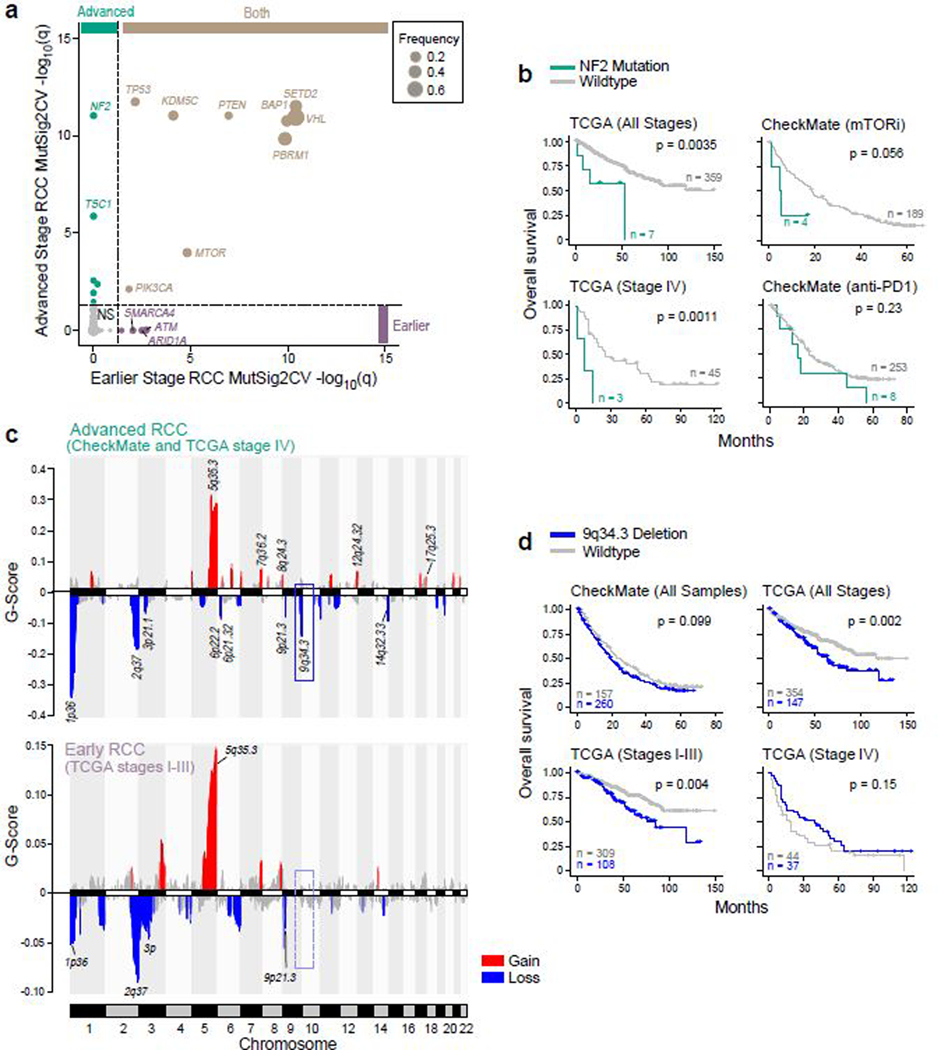
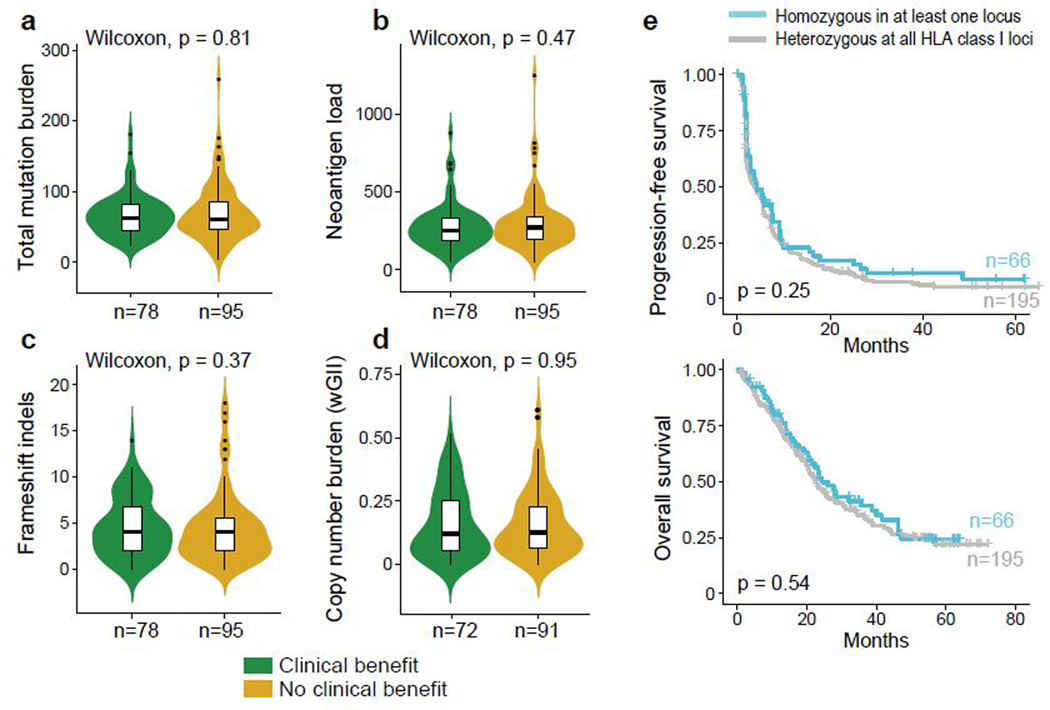
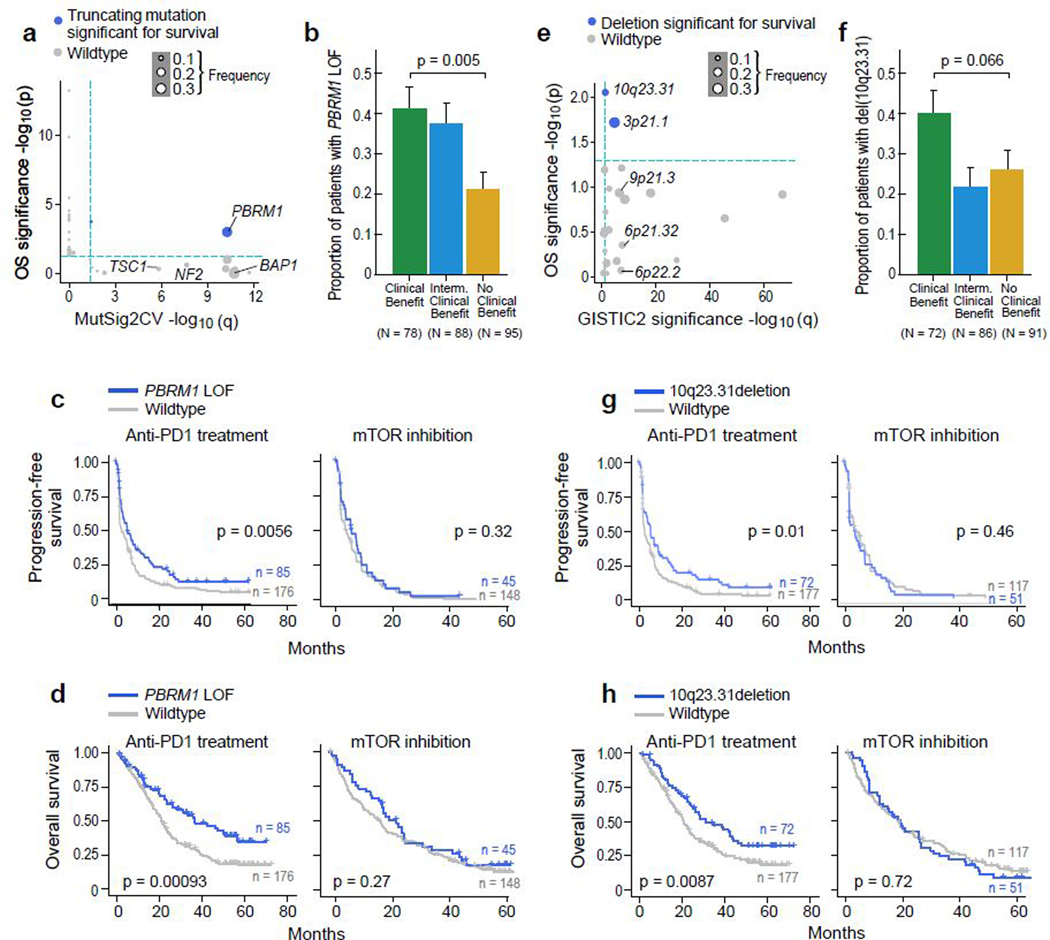
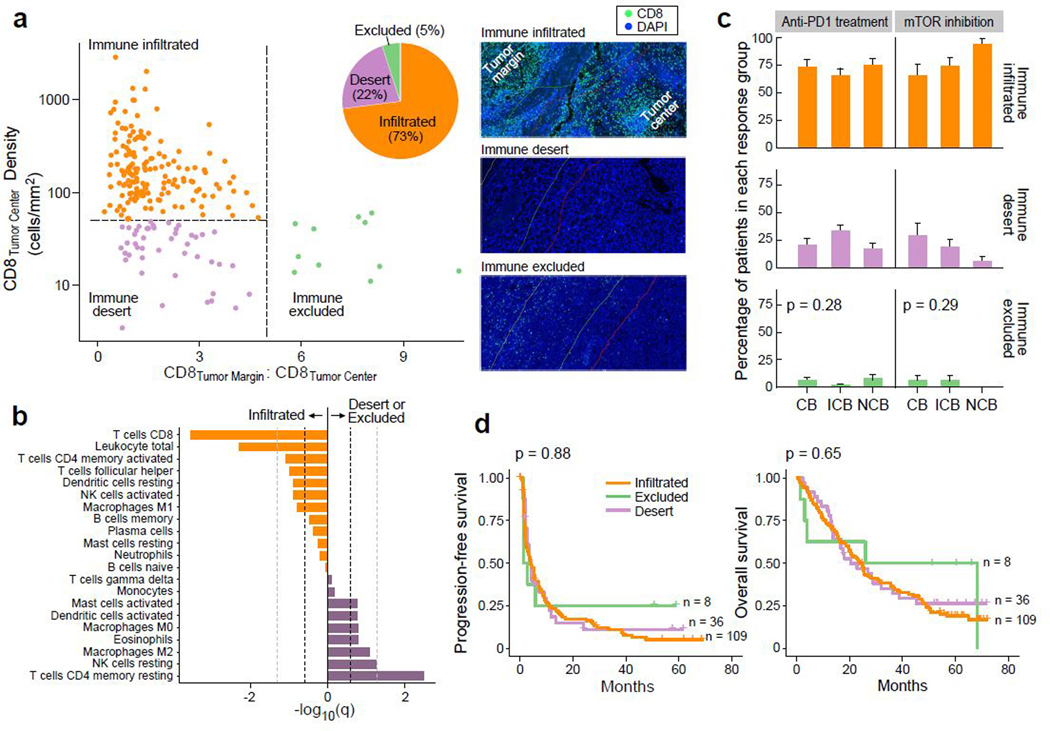
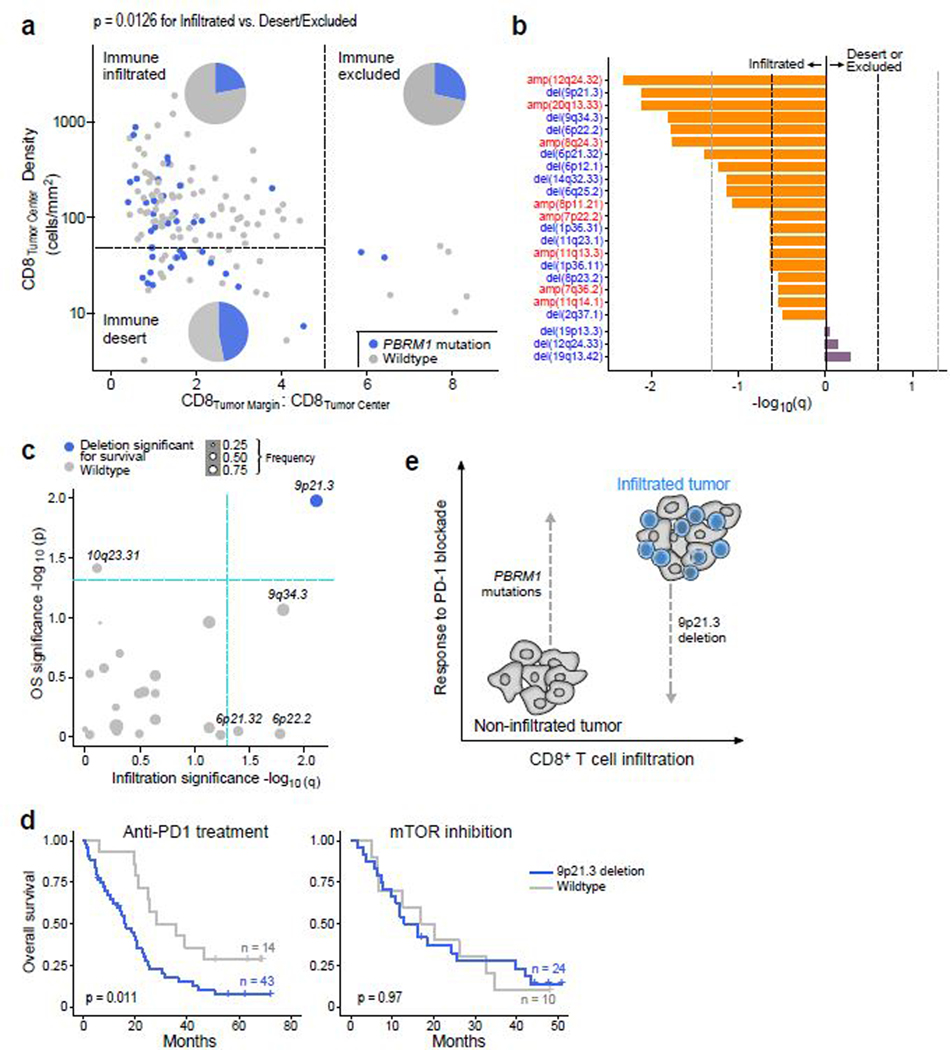
PD-1 blockade has transformed the management of advanced clear cell renal cell carcinoma (ccRCC), but the drivers and resistors of the PD-1 response remain incompletely elucidated. Here, we analyzed 592 tumors from patients with advanced ccRCC enrolled in prospective clinical trials of treatment with PD-1 blockade by whole-exome and RNA sequencing, integrated with immunofluorescence analysis, to uncover the immunogenomic determinants of the therapeutic response. Although conventional genomic markers (such as tumor mutation burden and neoantigen load) and the degree of CD8+ T cell infiltration were not associated with clinical response, we discovered numerous chromosomal alterations associated with response or resistance to PD-1 blockade. These advanced ccRCC tumors were highly CD8+ T cell infiltrated, with only 27% having a non-infiltrated phenotype. Our analysis revealed that infiltrated tumors are depleted of favorable PBRM1 mutations and enriched for unfavorable chromosomal losses of 9p21.3, as compared with non-infiltrated tumors, demonstrating how the potential interplay of immunophenotypes with somatic alterations impacts therapeutic efficacy.
Conflict of interest statement
COMPETING INTERESTS:
The other authors declare no potential conflicts of interest.
Figures
References
MAIN REFERENCES:
METHODS REFERENCES:
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
