

Comparison of Core Features in Four Developmental Encephalopathies in the Rett Natural History Study
- PMID: 32472944
- PMCID: PMC8882337
- DOI: 10.1002/ana.25797
Comparison of Core Features in Four Developmental Encephalopathies in the Rett Natural History Study
Abstract
Objective: Rett syndrome, CDKL5-deficiency disorder, FOXG1 disorder, and MECP2 duplication disorder are developmental encephalopathies with shared and distinct features. Although they are historically linked, no direct comparison has been performed. The first head-to-head comparison of clinical features in these conditions is presented.
Methods: Comprehensive clinical information was collected from 793 individuals enrolled in the Rett and Rett-Related Disorders Natural History Study. Clinical features including clinical severity, regression, and seizures were cross-sectionally compared between diagnoses to test the hypothesis that these are 4 distinct disorders.
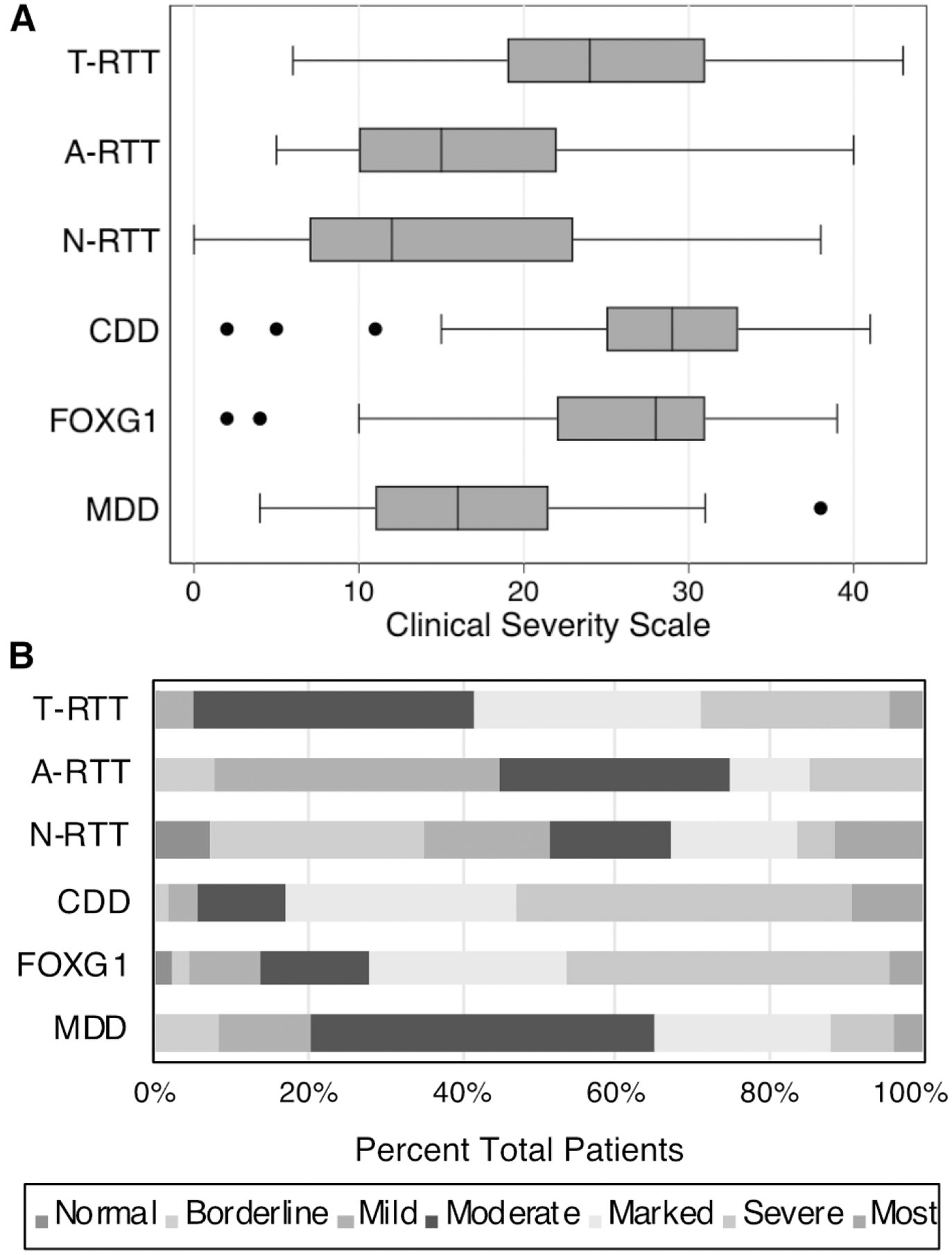
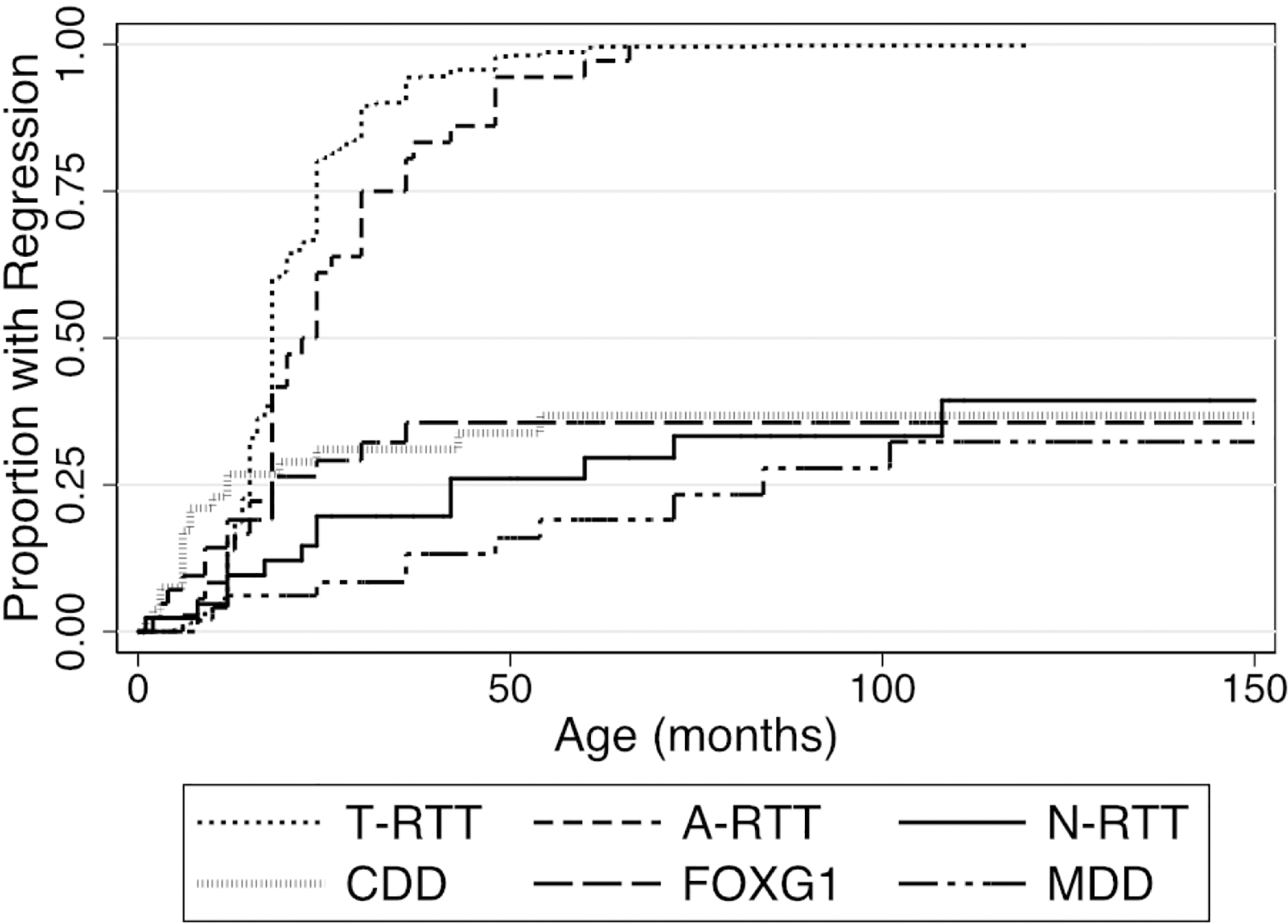
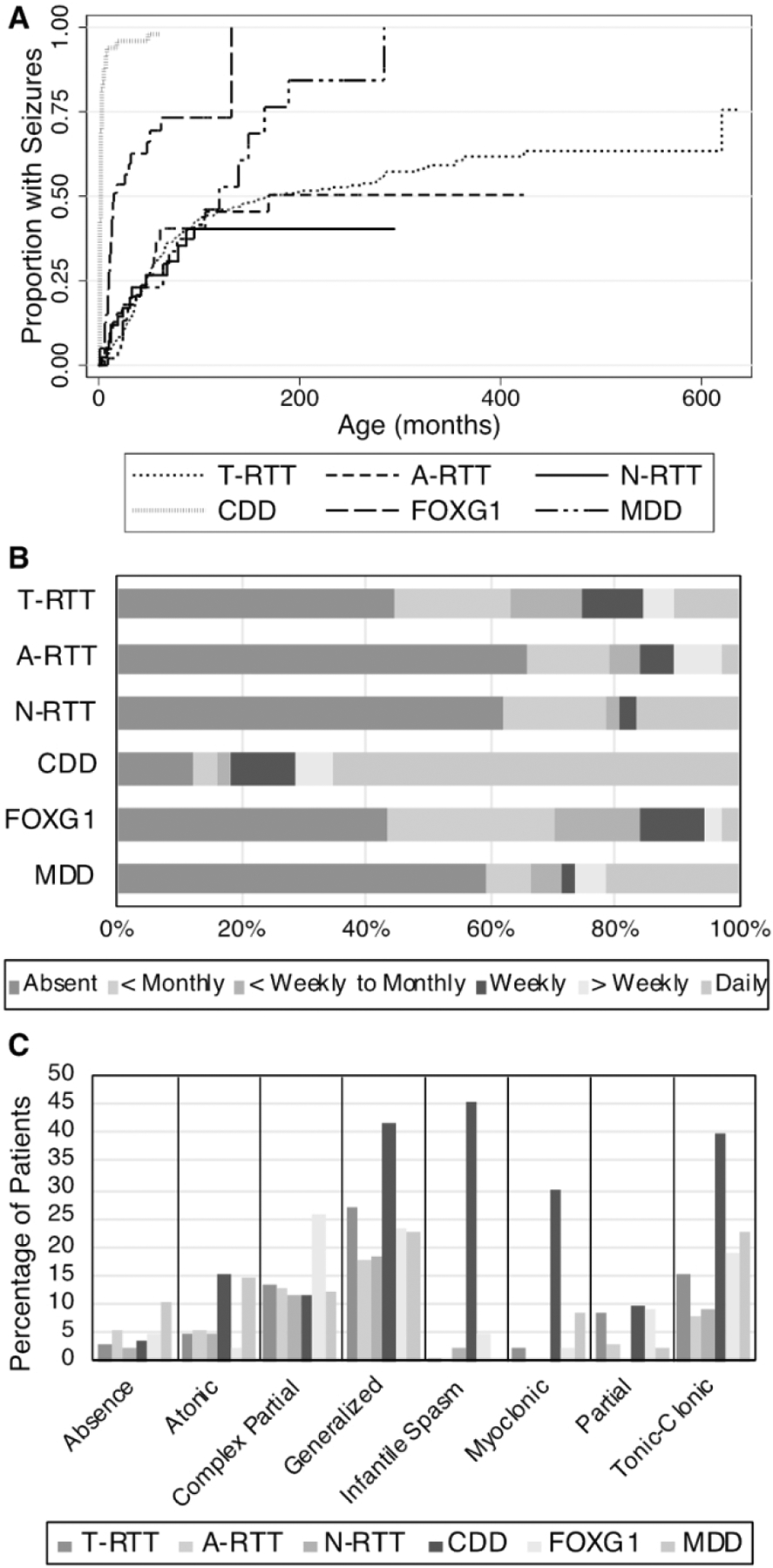
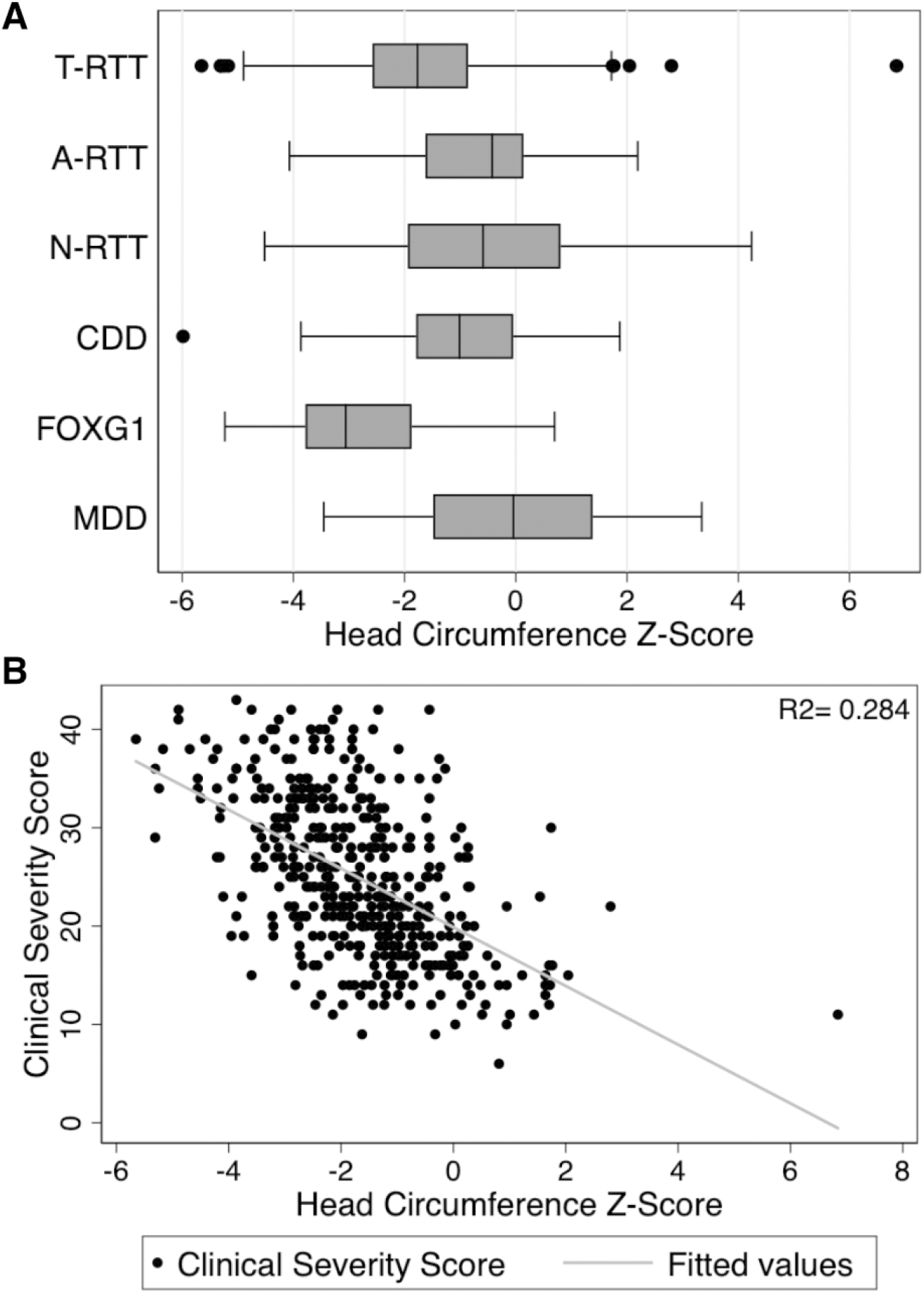
Results: Distinct patterns of clinical severity, seizure onset age, and regression were present. Individuals with CDKL5-deficency disorder were the most severely affected and had the youngest age at seizure onset (2 months), whereas children with MECP2 duplication syndrome had the oldest median age at seizure onset (64 months) and lowest severity scores. Rett syndrome and FOGX1 were intermediate in both features. Smaller head circumference correlates with increased severity in all disorders and earlier age at seizure onset in MECP2 duplication syndrome. Developmental regression occurred in all Rett syndrome participants (median = 18 months) but only 23 to 34% of the other disorders. Seizure incidence prior to the baseline visit was highest for CDKL5 deficiency disorder (96.2%) and lowest for Rett syndrome (47.5%). Other clinical features including seizure types and frequency differed among groups.
Interpretation: Although these developmental encephalopathies share many clinical features, clear differences in severity, regression, and seizures warrant considering them as unique disorders. These results will aid in the development of disease-specific severity scales, precise therapeutics, and future clinical trials. ANN NEUROL 2020;88:396-406.
© 2020 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
CCF, JS, DA, CG, AP, EDM, SP, JL, JN: Nothing to report
Figures
References
-
- Swaiman KF, Ashwal S, Ferriero DM, et al. Swaiman’s pediatric neurology : principles and practice [Internet]. 2018. Available from: https://www.worldcat.org/title/swaimans-pediatric-neurology-principles-a...
-
- Neul JL, Kaufmann WE, Glaze DG, et al. Rett Syndrome: Revised Diagnostic Criteria and Nomenclature [Internet]. Ann Neurol 2010;68(6):944–950.[cited 2018 Aug 8] Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3058521/pdf/nihms214759.pdf - PMC - PubMed
-
- Laurvick CL, de Klerk N, Bower C, et al. Rett syndrome in Australia: a review of the epidemiology. [Internet]. J. Pediatr 2006;148(3):347–52.[cited 2019 Jan 13] Available from: http://www.ncbi.nlm.nih.gov/pubmed/16615965 - PubMed
-
- Cuddapah VA, Pillai RB, Shekar KV, et al. Methyl-CpG-binding protein 2 (MEPC2) mutation type is associated with disease severity in Rett Syndrome HHS Public Access [Internet]. J Med Genet 2014;51(3):152–158.[cited 2019 Jan 13] Available from: http://mecp2.chw.edu.au - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- U54 HD083211/HD/NICHD NIH HHS/United States
- U54 HD061222/HD/NICHD NIH HHS/United States
- U54HD083211/Vanderbilt Intellectual and Developmental Disabilities Research Center/International
- 3 U54-HD061222-14S1/NIH National Institutes of Child Health and Disease/International
- U54 HD086984/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
