

Co-infections in people with COVID-19: a systematic review and meta-analysis
- PMID: 32473235
- PMCID: PMC7255350
- DOI: 10.1016/j.jinf.2020.05.046
Co-infections in people with COVID-19: a systematic review and meta-analysis
Abstract
Objectives: In previous influenza pandemics, bacterial co-infections have been a major cause of mortality. We aimed to evaluate the burden of co-infections in patients with COVID-19.
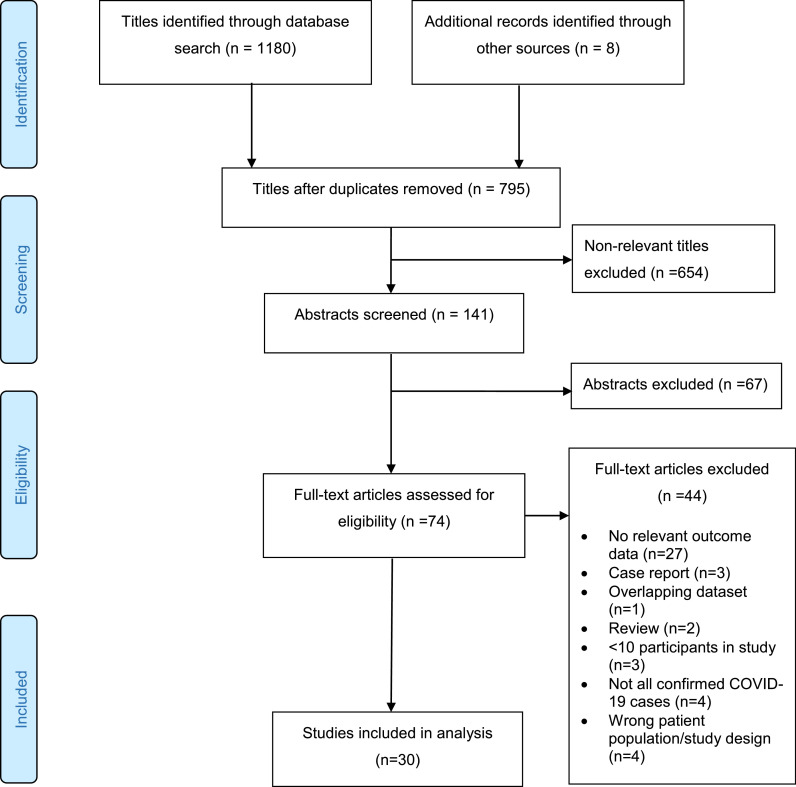
Methods: We systematically searched Embase, Medline, Cochrane Library, LILACS and CINAHL for eligible studies published from 1 January 2020 to 17 April 2020. We included patients of all ages, in all settings. The main outcome was the proportion of patients with a bacterial, fungal or viral co-infection. .
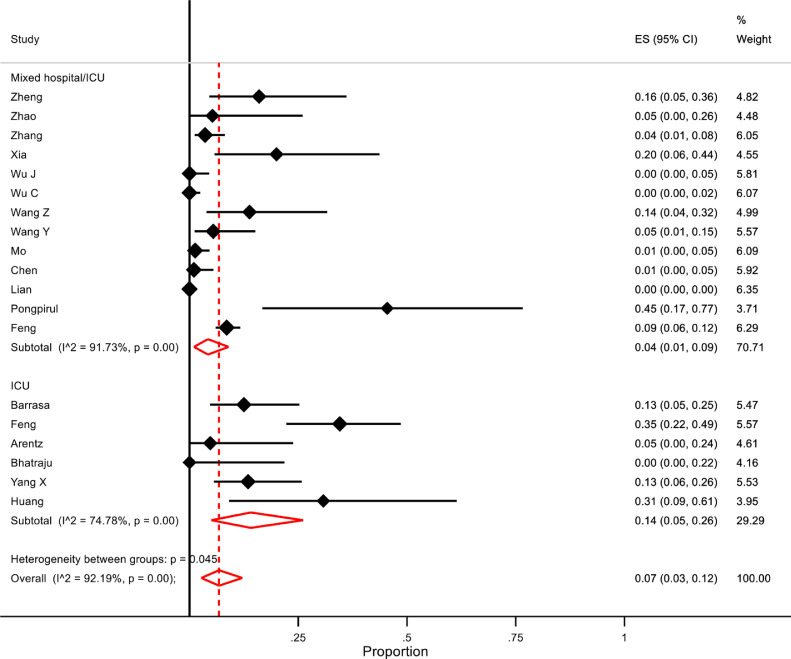
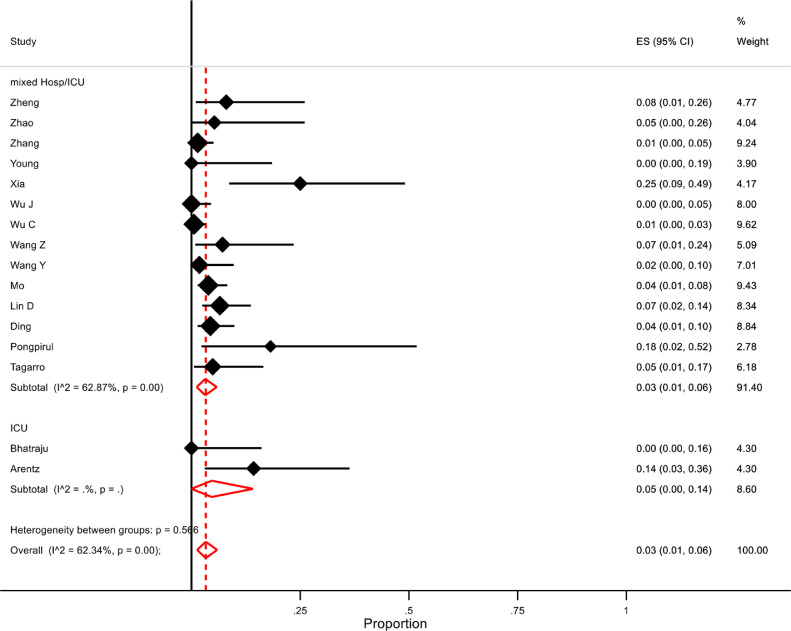
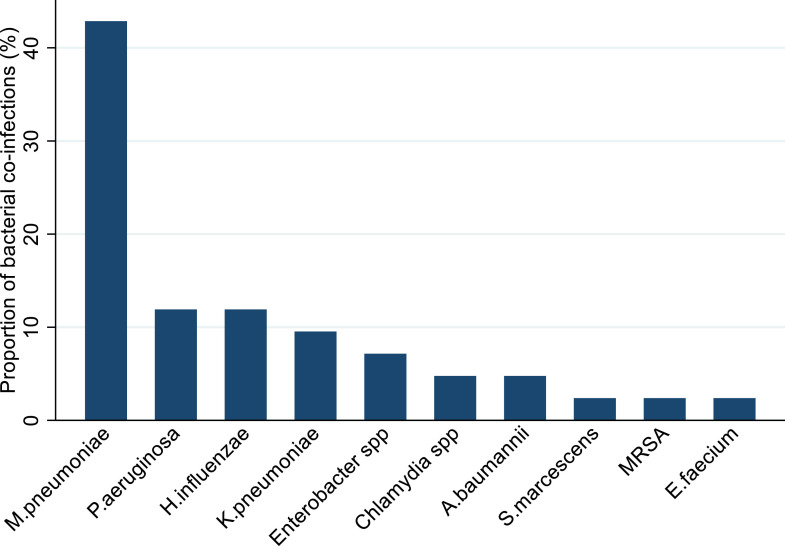
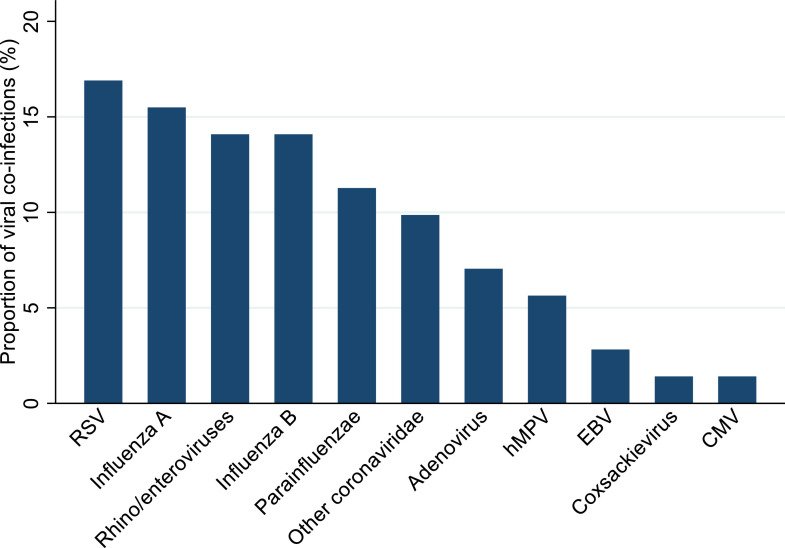
Results: Thirty studies including 3834 patients were included. Overall, 7% of hospitalised COVID-19 patients had a bacterial co-infection (95% CI 3-12%, n=2183, I2=92·2%). A higher proportion of ICU patients had bacterial co-infections than patients in mixed ward/ICU settings (14%, 95% CI 5-26, I2=74·7% versus 4%, 95% CI 1-9, I2= 91·7%). The commonest bacteria were Mycoplasma pneumonia, Pseudomonas aeruginosa and Haemophilus influenzae. The pooled proportion with a viral co-infection was 3% (95% CI 1-6, n=1014, I2=62·3%), with Respiratory Syncytial Virus and influenza A the commonest. Three studies reported fungal co-infections.
Conclusions: A low proportion of COVID-19 patients have a bacterial co-infection; less than in previous influenza pandemics. These findings do not support the routine use of antibiotics in the management of confirmed COVID-19 infection.
Keywords: COVID-19; Coinfection; Coronavirus; Meta-Analysis.
Copyright © 2020 The British Infection Association. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest LL, BL and VB declare no competing interests. WSL's institution has received unrestricted investigated-initiated research funding from Pfizer for an unrelated pneumonia cohort study in which he is the Chief Investigator.
Figures
Comment in
-
Early administered antibiotics do not impact mortality in critically ill patients with COVID-19.J Infect. 2020 Aug;81(2):e148-e149. doi: 10.1016/j.jinf.2020.06.004. Epub 2020 Jun 5. J Infect. 2020. PMID: 32512022 Free PMC article. No abstract available.
-
SARS-CoV-2 and co-infections detection in nasopharyngeal throat swabs of COVID-19 patients by metagenomics.J Infect. 2020 Aug;81(2):e175-e177. doi: 10.1016/j.jinf.2020.06.033. Epub 2020 Jun 17. J Infect. 2020. PMID: 32562797 Free PMC article. No abstract available.
-
Improving antibiotic stewardship in COVID-19: Bacterial co-infection is less common than with influenza.J Infect. 2020 Sep;81(3):e55-e57. doi: 10.1016/j.jinf.2020.06.056. Epub 2020 Jun 25. J Infect. 2020. PMID: 32593654 Free PMC article. No abstract available.
-
COVID-19 and TB co-infection - 'Finishing touch'' in perfect recipe to 'severity' or 'death'.J Infect. 2020 Sep;81(3):e39-e40. doi: 10.1016/j.jinf.2020.06.062. Epub 2020 Jun 29. J Infect. 2020. PMID: 32610112 Free PMC article. No abstract available.
-
COVID-19 associated invasive candidiasis.J Infect. 2021 Feb;82(2):e45-e46. doi: 10.1016/j.jinf.2020.08.005. Epub 2020 Aug 7. J Infect. 2021. PMID: 32771402 Free PMC article. No abstract available.
-
Emergence of co-infection of COVID-19 and dengue: A serious public health threat.J Infect. 2020 Dec;81(6):e16-e18. doi: 10.1016/j.jinf.2020.08.009. Epub 2020 Aug 12. J Infect. 2020. PMID: 32800797 Free PMC article. No abstract available.
-
Low incidence of co-infection, but high incidence of ICU-acquired infections in critically ill patients with COVID-19.J Infect. 2021 Feb;82(2):e20-e21. doi: 10.1016/j.jinf.2020.09.010. Epub 2020 Sep 19. J Infect. 2021. PMID: 32956729 Free PMC article. No abstract available.
-
Co-infection in COVID-19, a cohort study.J Infect. 2021 Mar;82(3):414-451. doi: 10.1016/j.jinf.2020.10.006. Epub 2020 Oct 8. J Infect. 2021. PMID: 33039502 Free PMC article. No abstract available.
-
The presence of Pneumocystis jirovecii in critically ill patients with COVID-19.J Infect. 2021 Apr;82(4):84-123. doi: 10.1016/j.jinf.2020.10.034. Epub 2020 Nov 4. J Infect. 2021. PMID: 33157150 Free PMC article. No abstract available.
-
SARS-CoV-2 and superimposed infection by trichomonads.J Infect. 2021 Mar;82(3):e22-e23. doi: 10.1016/j.jinf.2020.11.038. Epub 2020 Nov 30. J Infect. 2021. PMID: 33271170 Free PMC article. No abstract available.
-
Co-infection of chlamydia pneumoniae and mycoplasma pneumoniae with SARS-CoV-2 is associated with more severe features.J Infect. 2021 Apr;82(4):e4-e7. doi: 10.1016/j.jinf.2021.01.009. Epub 2021 Jan 19. J Infect. 2021. PMID: 33482238 Free PMC article. No abstract available.
-
Mucormycosis-A serious threat in the COVID-19 pandemic?J Infect. 2021 Aug;83(2):237-279. doi: 10.1016/j.jinf.2021.05.015. Epub 2021 May 21. J Infect. 2021. PMID: 34029629 Free PMC article. No abstract available.
-
The impact of secondary infections in COVID-19 critically ill patients.J Infect. 2022 Jun;84(6):e116-e117. doi: 10.1016/j.jinf.2022.03.017. Epub 2022 Mar 18. J Infect. 2022. PMID: 35314266 Free PMC article. No abstract available.
-
The risk of methicillin-resistant Staphylococcus aureus infection following COVID-19 and influenza: A retrospective cohort study from the TriNetX network.J Infect. 2023 Mar;86(3):256-308. doi: 10.1016/j.jinf.2023.01.006. Epub 2023 Jan 9. J Infect. 2023. PMID: 36632945 Free PMC article. No abstract available.
References
-
- World Health Organization. Coronavirus Disease (COVID-19) pandemicAvailable from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 13 May 2020
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
