

Omega-3 fatty acid exposure with a low-fat diet in patients with past hypertriglyceridemia-induced acute pancreatitis; an exploratory, randomized, open-label crossover study
- PMID: 32473640
- PMCID: PMC7260759
- DOI: 10.1186/s12944-020-01295-7
Omega-3 fatty acid exposure with a low-fat diet in patients with past hypertriglyceridemia-induced acute pancreatitis; an exploratory, randomized, open-label crossover study
Abstract
Background: Omega-3 fatty acids (OM3-FAs) are recommended with a low-fat diet for severe hypertriglyceridemia (SHTG), to reduce triglycerides and acute pancreatitis (AP) risk. A low-fat diet may reduce pancreatic lipase secretion, which is required to absorb OM3-ethyl esters (OM3-EEs), but not OM3-carboxylic acids (OM3-CAs).
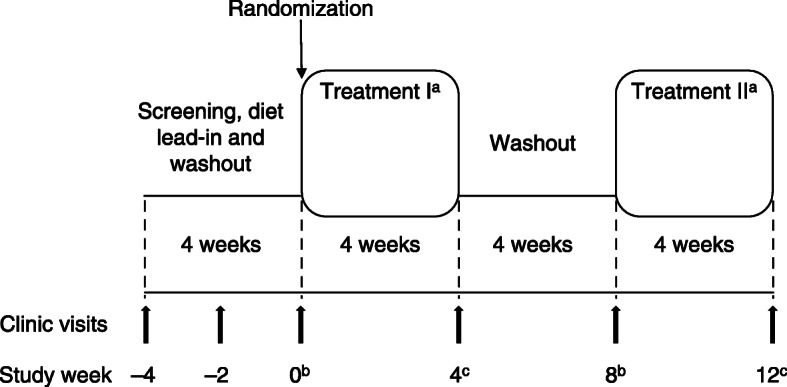
Methods: In this exploratory, randomized, open-label, crossover study, 15 patients with SHTG and previous AP were instructed to take OM3-CA (2 g or 4 g) and OM3-EE 4 g once daily for 4 weeks, while adhering to a low-fat diet. On day 28 of each treatment phase, a single dose was administered in the clinic with a liquid low-fat meal, to assess 24-h plasma exposure. Geometric least-squares mean ratios were used for between-treatment comparisons of baseline (day 0)-adjusted area under the plasma concentration versus time curves (AUC0-24) and maximum plasma concentrations (Cmax) for eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).
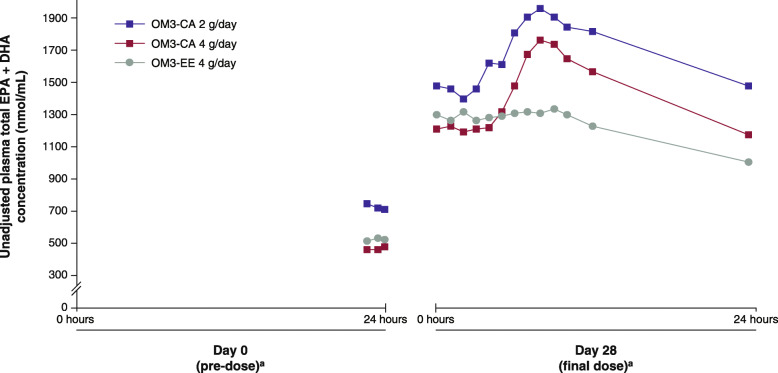
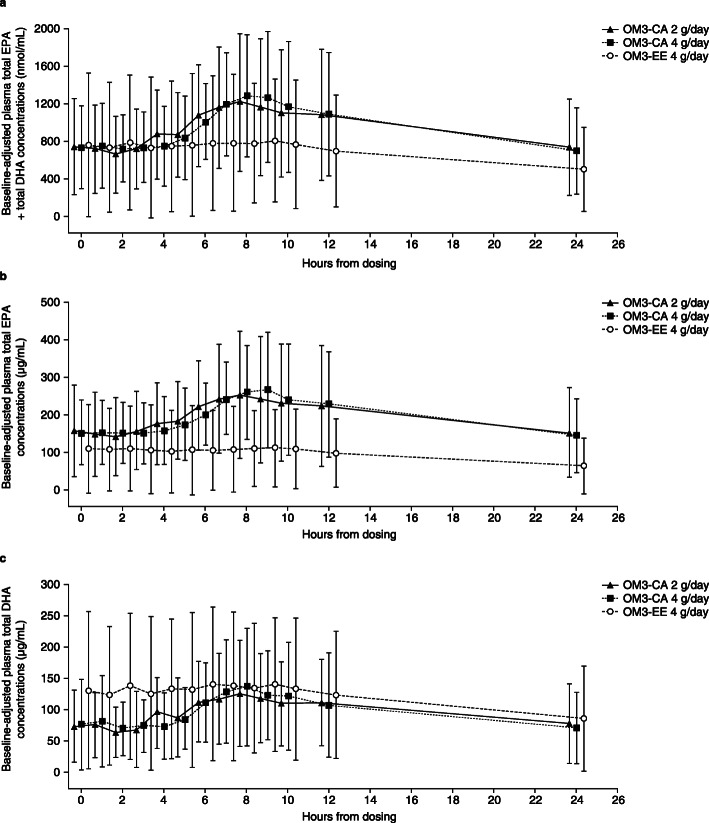
Results: Before initiating OM3-FA treatment, mean baseline fasting plasma EPA + DHA concentrations (nmol/mL) were 723 for OM3-CA 2 g, 465 for OM3-CA 4 g and 522 for OM3-EE 4 g. At week 4, mean pre-dose fasting plasma EPA + DHA concentrations increased by similar amounts (+ 735 - + 768 nmol/mL) for each treatment. During the 24-h exposure assessment (day 28), mean plasma EPA + DHA increased from pre-dose to the maximum achieved concentration by + 32.7%, + 45.8% and + 3.1% with single doses of OM3-CA 2 g, OM3-CA 4 g and OM3-EE 4 g, respectively. Baseline-adjusted AUC0-24 was 60% higher for OM3-CA 4 g than for OM3-EE 4 g and baseline-adjusted Cmax was 94% higher (both non-significant).
Conclusions: Greater 24-h exposure of OM3-CA versus OM3-EE was observed for some parameters when administered with a low-fat meal at the clinic on day 28. However, increases in pre-dose fasting plasma EPA + DHA over the preceding 4-week dosing period were similar between treatments, leading overall to non-significant differences in baseline (day 0)-adjusted AUC0-24 and Cmax EPA + DHA values. It is not clear why the greater 24-h exposure of OM3-CA versus OM3-EE observed with a low-fat meal did not translate into significantly higher pre-dose fasting levels of DHA + EPA with longer-term use.
Trial registration: ClinicalTrials.gov, NCT02189252, Registered 23 June 2014.
Keywords: Clinical trials; Docosahexaenoic acid; Eicosapentaenoic acid; Fish oil; Omega-3 carboxylic acids; Omega-3 ethyl esters; Omega-3 fatty acids; Pharmacokinetics; Triglycerides; Viscosity.
Conflict of interest statement
MD was the Founder and Chief Medical Officer of Omthera (manufacturer of Epanova), prior to its acquisition by AstraZeneca. RLD was employed by ICON Clinical Services during the bulk of the manuscript preparation, and is currently an employee and stock shareholder of Amarin Pharma, Inc. RLD has received grant support from Omthera and AstraZeneca. DG has received grant support from AstraZeneca and GlaxoSmithKline. JO and CN are employees of AstraZeneca. MK and HY were employees of AstraZeneca when the study was conducted.
Figures
References
-
- Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, Wiklund O, et al. ESC/EAS guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European atherosclerosis society (EAS) Eur Heart J. 2011;32:1769–1818. doi: 10.1093/eurheartj/ehr158. - DOI - PubMed
-
- Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001;285:2486–97. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
