

Estimation of Renin-Angiotensin-Aldosterone-System (RAAS)-Inhibitor effect on COVID-19 outcome: A Meta-analysis
- PMID: 32474043
- PMCID: PMC7255761
- DOI: 10.1016/j.jinf.2020.05.052
Estimation of Renin-Angiotensin-Aldosterone-System (RAAS)-Inhibitor effect on COVID-19 outcome: A Meta-analysis
Abstract
Background and rationale: Some studies of hospitalized patients suggested that the risk of death and/or severe illness due to COVID-19 is not associated with the use of angiotensin-converting enzyme inhibitors (ACEIs) and/or angiotensin II receptor type 1 blockers (ARBs). Nevertheless, some controversy still exists and there is limited information of the ACEIs/ARBs effect size on COVID-19 prognosis.
Aim and methods: We aimed to measure the effect of ACEIs and/or ARBs on COVID-19 severe clinical illness by a meta-analysis. Literature search included all studies published since the COVID-19 outbreak began (December 2019) until May 9, 2020. We analyzed information from studies that included tested COVID-19 patients with arterial hypertension as comorbidity prior to hospital admission and history of taking ACEIs, ARBs, or ACEIs/ARBs.
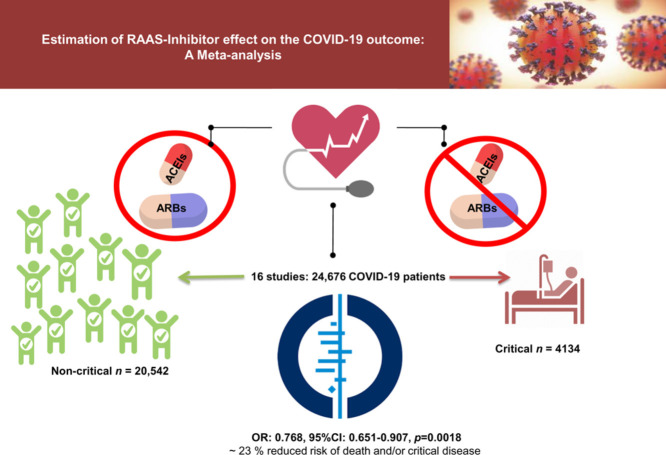
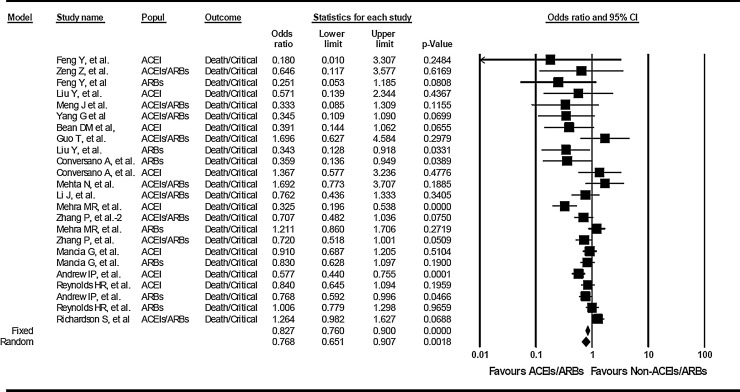
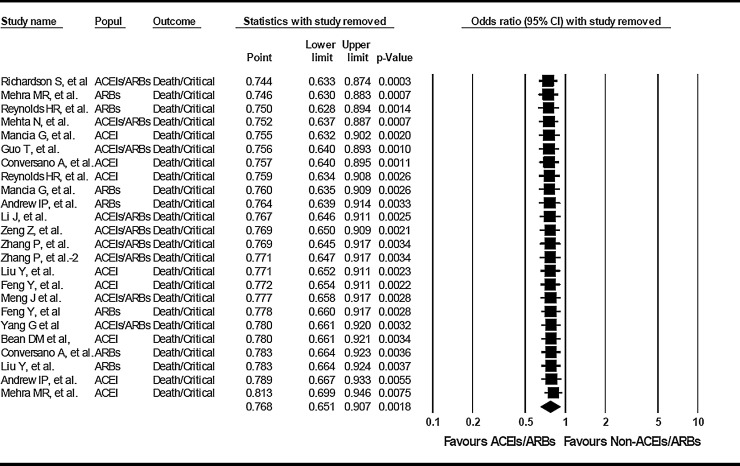
Results: We included 16 studies that involved 24,676 COVID-19 patients, and we compared patients with critical (n = 4134) vs. non-critical (n = 20,542) outcomes. The overall assessment by estimating random effects shows that the use of ACEIs/ARBs is not associated with higher risk of in-hospital-death and/or severe illness among hypertensive patients with COVID-19 infection. On the contrary, effect estimate shows an overall protective effect of RAAS inhibitors/blockers (ACEIs, ARBs, and/or ACEIs/ARBs) with ∼ 23 % reduced risk of death and/or critical disease (OR: 0.768, 95%CI: 0.651-0.907, p=0.0018). The use of ACEIs (OR:0.652, 95%CI:0.478-0.891, p=0.0072) but not ACEIs/ARBs (OR:0.867, 95%CI:0.638-1.179, p =NS) or ARBs alone (OR:0.810, 95%CI:0.629-1.044, p=NS) may explain the overall protection displayed by RAAS intervention combined.
Conclusion: RAAS inhibitors might be associated with better COVID-19 prognosis.
Keywords: Angiotensin II receptor type 1 blockers; Angiotensin II-converting enzyme inhibitors; COVID-19; RAAS inhibitors; cardiovascular disease; diabetes; hypertension; prognosis.
Copyright © 2020. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest CJP: no conflict of interest to declare. SS: no conflict of interest to declare
Figures
Similar articles
-
A systematic review and meta-analysis of the use of renin-angiotensin system drugs and COVID-19 clinical outcomes: What is the evidence so far?Pharmacol Res Perspect. 2020 Dec;8(6):e00666. doi: 10.1002/prp2.666. Pharmacol Res Perspect. 2020. PMID: 33084232 Free PMC article.
-
Association of Renin-Angiotensin System Inhibitors With Severity or Risk of Death in Patients With Hypertension Hospitalized for Coronavirus Disease 2019 (COVID-19) Infection in Wuhan, China.JAMA Cardiol. 2020 Jul 1;5(7):825-830. doi: 10.1001/jamacardio.2020.1624. JAMA Cardiol. 2020. PMID: 32324209 Free PMC article.
-
A Retrospective Study from 2 Centers in China on the Effects of Continued Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers in Patients with Hypertension and COVID-19.Med Sci Monit. 2020 Sep 24;26:e926651. doi: 10.12659/MSM.926651. Med Sci Monit. 2020. PMID: 32969367 Free PMC article.
-
Renin-angiotensin system inhibitors and the severity of coronavirus disease 2019 in Kanagawa, Japan: a retrospective cohort study.Hypertens Res. 2020 Nov;43(11):1257-1266. doi: 10.1038/s41440-020-00535-8. Epub 2020 Aug 21. Hypertens Res. 2020. PMID: 32820236
-
Renin-Angiotensin System Blockade and Mortality in Patients With Hypertension and COVID-19 Infection.J Cardiovasc Pharmacol Ther. 2020 Nov;25(6):503-507. doi: 10.1177/1074248420947628. Epub 2020 Aug 4. J Cardiovasc Pharmacol Ther. 2020. PMID: 32748634 Free PMC article. Review.
Cited by
-
Mortality and Disease Severity Among COVID-19 Patients Receiving Renin-Angiotensin System Inhibitors: A Systematic Review and Meta-analysis.Am J Cardiovasc Drugs. 2020 Dec;20(6):571-590. doi: 10.1007/s40256-020-00439-5. Epub 2020 Sep 12. Am J Cardiovasc Drugs. 2020. PMID: 32918209 Free PMC article.
-
Outcomes of renin-angiotensin-aldosterone system blockers in patients with COVID-19: a systematic review and meta-analysis.Eur Heart J Cardiovasc Pharmacother. 2020 Sep 1;6(5):335-337. doi: 10.1093/ehjcvp/pvaa074. Eur Heart J Cardiovasc Pharmacother. 2020. PMID: 32671399 Free PMC article. No abstract available.
-
Influence of angiotensin converting enzyme inhibitors/angiotensin receptor blockers on the risk of all-cause mortality and other clinical outcomes in patients with confirmed COVID-19: A systemic review and meta-analysis.J Clin Hypertens (Greenwich). 2021 Sep;23(9):1651-1663. doi: 10.1111/jch.14329. Epub 2021 Jul 28. J Clin Hypertens (Greenwich). 2021. PMID: 34320275 Free PMC article.
-
Prospective meta-analysis protocol on randomised trials of renin-angiotensin system inhibitors in patients with COVID-19: an initiative of the International Society of Hypertension.BMJ Open. 2021 Feb 16;11(2):e043625. doi: 10.1136/bmjopen-2020-043625. BMJ Open. 2021. PMID: 33593784 Free PMC article.
-
An umbrella review and meta-analysis of renin-angiotensin system drugs use and COVID-19 outcomes.Eur J Clin Invest. 2023 Feb;53(2):e13888. doi: 10.1111/eci.13888. Epub 2022 Oct 19. Eur J Clin Invest. 2023. PMID: 36205627 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
