

Clinical characteristics and chest CT imaging features of critically ill COVID-19 patients
- PMID: 32474629
- PMCID: PMC7260469
- DOI: 10.1007/s00330-020-06955-x
Clinical characteristics and chest CT imaging features of critically ill COVID-19 patients
Abstract
Objectives: To compare clinical, laboratory, and chest computed tomography (CT) findings in critically ill patients diagnosed with coronavirus disease 2019 (COVID-19) who survived and who died.
Methods: This retrospective study reviewed 60 critically ill patients (43 males and 17 females, mean age 64.4 ± 11.0 years) with COVID-19 pneumonia who were admitted to two different clinical centers. Their clinical and medical records were analyzed, and the chest CT images were assessed to determine the involvement of lobes and the distribution of lesions in the lungs between the patients who recovered from the illness and those who died.
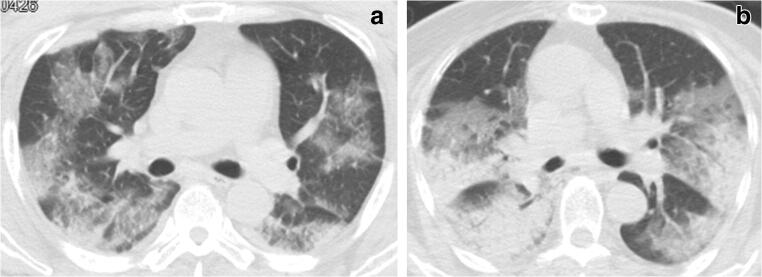
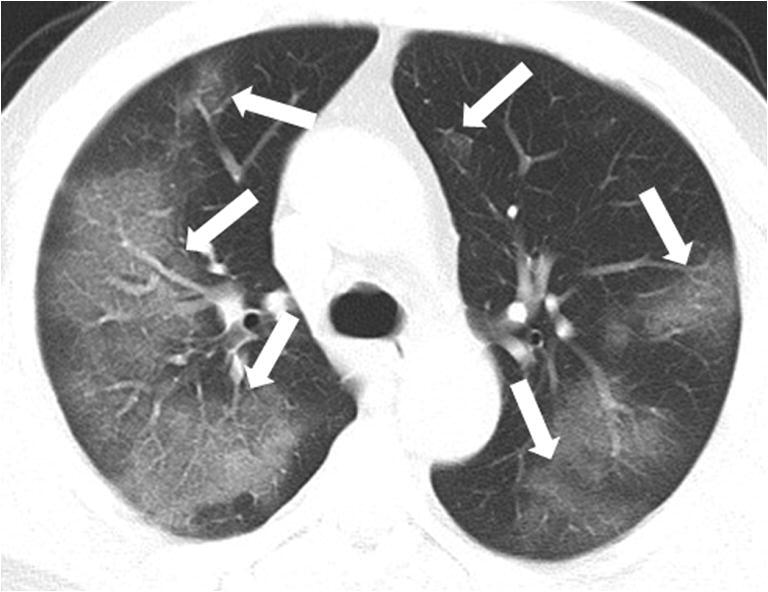
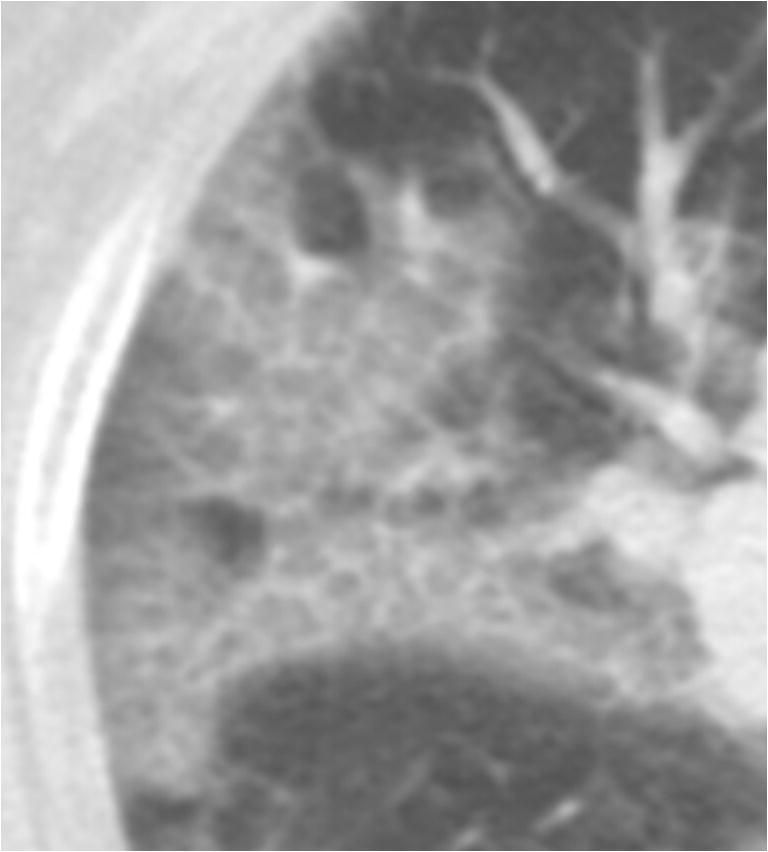
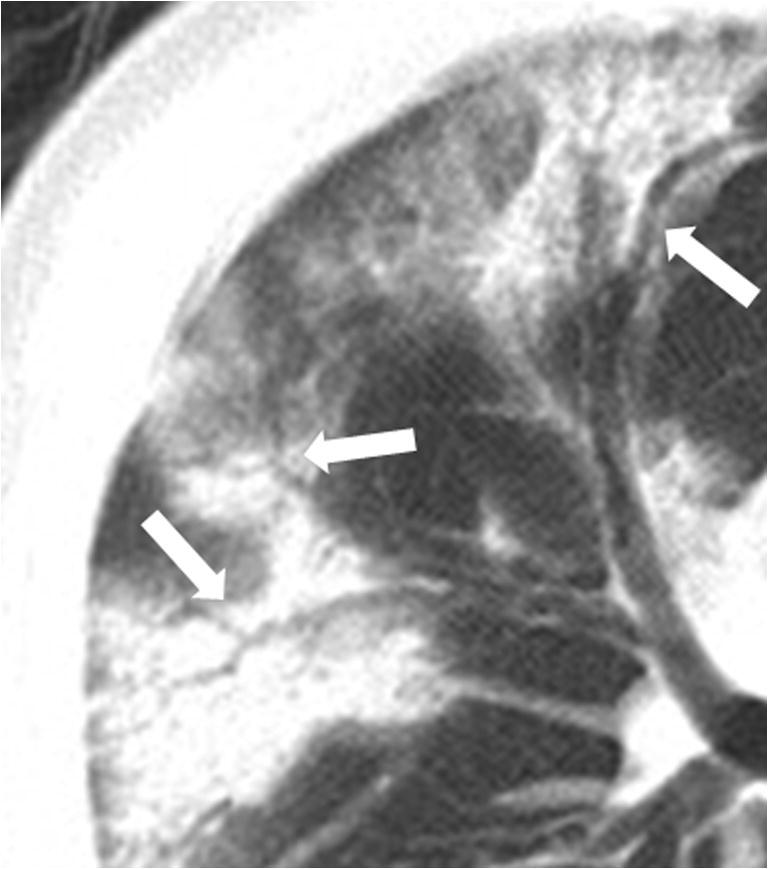
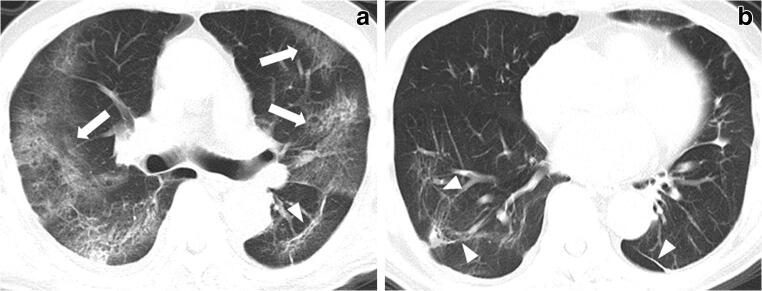
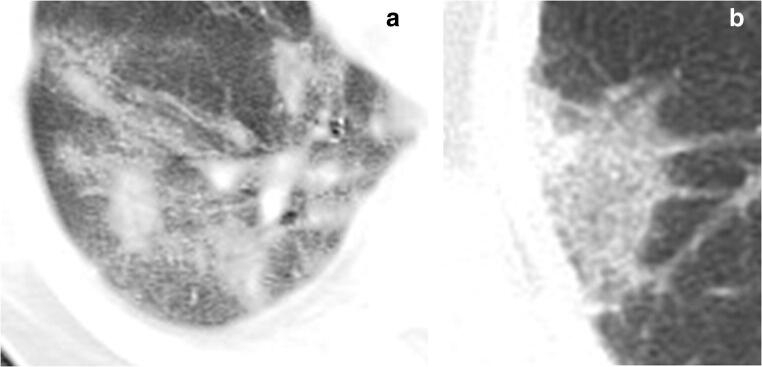
Results: Compared with recovered patients (50/60, 83%), deceased patients (10/60, 17%) were older (mean age, 70.6 vs. 62.6 years, p = 0.044). C-reactive protein (CRP) (110.8 ± 26.3 mg/L vs 63.0 ± 50.4 mg/L, p < 0.001) and neutrophil-to-lymphocyte ratio (NLR) (18.7 ± 16.6 vs 8.4 ± 7.5, p = 0.030) were significantly elevated in the deceased as opposed to the recovered. Medial or parahilar area involvement was observed in all the deceased patients (10/10, 100%), when compared to only 54% (27/50) in the recovered. Ground-glass opacities (97%), crazy-paving pattern (92%), and air bronchogram (93%) were the most common radiological findings. There was significant difference in diabetes (p = 0.025) and emphysema (p = 0.013), and the odds ratio on a deceased patient having diabetes and emphysema was 6 times and 21 times the odds ratio on a recovered patient having diabetes and emphysema, respectively.
Conclusions: Older patients with comorbidities such as diabetes and emphysema, and higher CRP and NLRs with diffuse lung involvement were more likely to die of COVID-19.
Key points: • Almost all patients critically ill with COVID-19 pneumonia had five lung lobes involved. • Medial or parahilar area involvement and degree of lung involvement were more serious in the deceased patients when compared with those who recovered from treatment. • Chronic lung disease, e.g., emphysema, diabetes, and higher serum CRP and NLR characterized patients who died of COVID-19.
Keywords: Comorbidity; Computed tomography; Coronavirus infections; Pneumonia; X-ray.
Conflict of interest statement
The authors declare no conflict of interest in this work.
Figures
References
-
- World Health Organization (2020) Novel coronavirus (2019-nCoV) situation report-75. https://www.who.int/docs/default-source/coronaviruse/20200302-sitrep-75-...
-
- Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Control and Prevention (2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 41(2):145–151 - PubMed
-
- Liu Y, Sun W, Li J, et al (2020) Clinical features and progression of acute respiratory distress syndrome in coronavirus disease 2019. medRxiv. 02.17.20024166
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
