

Impact of Formulary Restrictions on Antiepileptic Drug Dispensation Outcomes
- PMID: 32474812
- PMCID: PMC7606428
- DOI: 10.1007/s40120-020-00195-3
Impact of Formulary Restrictions on Antiepileptic Drug Dispensation Outcomes
Abstract
Introduction: The aim of this analysis was to assess the relationship between formulary restrictions and antiepileptic drug (AED) dispensation in patients with focal seizure (FS).
Study design: A retrospective cohort analysis was conducted using data from Symphony Health's Integrated Dataverse® (1 April 2015-30 June 2018).
Methods: This study included two patient populations: the overall patient population (N = 54,097) and a pediatric population (< 18 years) (N = 12,610). Cohorts were defined based on approval or rejection of the index AED claim. Study outcomes were prescription life cycle analysis, proportion of patients with dispensation, time to dispensation, and likelihood of successful dispensation. A multivariable Cox proportional hazards model was estimated to study the association between formulary restriction and likelihood of successful AED dispensation.
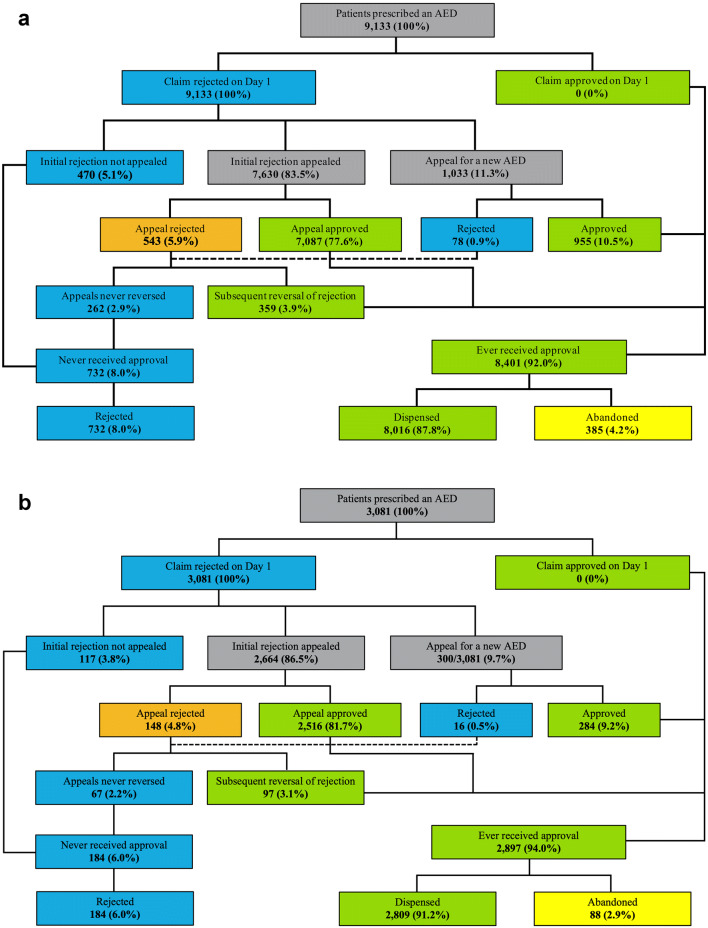
Results: Among patients in the overall population with a rejected claim (n = 9133), 8.0% did not receive any AED and 77.6% received approval for the index AED following an appeal. Among the pediatric patients with a rejected claim (n = 3081), 6.0% did not receive any AED and 81.7% received approval for the index AED after an appeal. In both populations, formulary restrictions were associated with significant delays in index AED dispensation (6.9 and 5.3 days, respectively; P < 0.0001 for each population), compared to approved AED claims. In the overall and pediatric populations, formulary-related rejections of AEDs were associated with a 35% (hazard ratio [HR] 0.65; 95% confidence interval [CI] 0.64-0.66; P < 0.0001) and 27% (HR 0.73; 95% CI 0.69-0.76; P < 0.0001) lower likelihood of successful dispensation of the index AED, respectively.
Conclusions: Formulary restrictions of AEDs were associated with significant delays in treatment and significantly lower likelihood of successful AED dispensation in patients with FS.
Keywords: Antiepileptic drug; Dispensation; Focal seizure; Formulary restriction; Treatment delay.
Plain language summary
Formulary restrictions on antiepileptic drugs (AEDs) are adopted by payers in the USA to guide the use of therapies and contain the costs of care. However, formulary restrictions on AEDs are inconsistent with the American Epilepsy Society position statement that indicates patients with epilepsy must have unrestricted access to all AEDs. This retrospective cohort analysis of open-source claims data assessed the effects of formulary restrictions on AED dispensation in patients with focal seizure (FS). Findings showed that formulary-related rejections of AED claims were associated with significant delays in treatment initiation and a significantly lower likelihood of successful AED dispensation. The treatment delays associated with formulary restrictions on AEDs may have a negative clinical and economic impact on patients with epilepsy and the healthcare system. Approximately 80% of rejected initial claims were reversed after an appeal. Claim denials and appeals represent an unnecessary administrative burden on physicians’ practices. Further studies are required to identify the patient, physician, or payer factors that drive the delay in access to AEDs among patients with FS.
Conflict of interest statement
Darshan Mehta is an employee of Sunovion Pharmaceuticals Inc. Andrew Lee was an employee of Sunovion Pharmaceuticals Inc. at the time of conducting the study; he is currently an employee of Vertex Pharmaceuticals. Matthew Davis is an employee of Medicus Economics, LLC, which received funding from the study sponsor to participate in this research. Andrew J Epstein is an employee of Medicus Economics, LLC, which received funding from the study sponsor to participate in this research.
Figures



Similar articles
-
Impact of formulary-related pharmacy claim rejections of cariprazine on health care utilization and treatment patterns among patients with bipolar I disorder.J Manag Care Spec Pharm. 2024 Feb 3;30(2):118-128. doi: 10.18553/jmcp.2024.30.2.118. J Manag Care Spec Pharm. 2024. PMID: 38308622 Free PMC article.
-
Impact of Early Initiation of Eslicarbazepine Acetate on Economic Outcomes Among Patients with Focal Seizure: Results from Retrospective Database Analyses.Neurol Ther. 2020 Dec;9(2):585-598. doi: 10.1007/s40120-020-00211-6. Epub 2020 Sep 19. Neurol Ther. 2020. PMID: 32949379 Free PMC article.
-
Current state of the union of epilepsy care in the United States: Antiepileptic drugs - An introduction to the Connectors Project.Epilepsy Behav. 2018 Mar;80:98-103. doi: 10.1016/j.yebeh.2017.12.026. Epub 2018 Feb 2. Epilepsy Behav. 2018. PMID: 29414565
-
Rapid versus slow withdrawal of antiepileptic drugs.Cochrane Database Syst Rev. 2020 Jan 23;1(1):CD005003. doi: 10.1002/14651858.CD005003.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Jan 10;1:CD005003. doi: 10.1002/14651858.CD005003.pub4. PMID: 31990368 Free PMC article. Updated.
-
Topiramate versus carbamazepine monotherapy for epilepsy: an individual participant data review.Cochrane Database Syst Rev. 2019 Jun 24;6(6):CD012065. doi: 10.1002/14651858.CD012065.pub3. Cochrane Database Syst Rev. 2019. PMID: 31233229 Free PMC article.
Cited by
-
Influence of prior authorization requirements on provider clinical decision-making.Am J Manag Care. 2023 Jul;29(7):331-337. doi: 10.37765/ajmc.2023.89394. Am J Manag Care. 2023. PMID: 37523751 Free PMC article.
-
The Impact of Insurance Restrictions in Newly Diagnosed Individuals With Multiple Sclerosis.Int J MS Care. 2024 Jan-Feb;26(1):17-21. doi: 10.7224/1537-2073.2022-069. Epub 2024 Jan 5. Int J MS Care. 2024. PMID: 38213675 Free PMC article.
-
Payer approval and rejection of oral anticoagulant prescriptions and prescription abandonment patterns among patients with venous thromboembolism.J Manag Care Spec Pharm. 2024 May;30(5):441-455. doi: 10.18553/jmcp.2024.23194. Epub 2024 Jan 26. J Manag Care Spec Pharm. 2024. PMID: 38277234 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
