Automated syndrome diagnosis by three-dimensional facial imaging
- PMID: 32475986
- PMCID: PMC7521994
- DOI: 10.1038/s41436-020-0845-y
Automated syndrome diagnosis by three-dimensional facial imaging
Abstract
Purpose: Deep phenotyping is an emerging trend in precision medicine for genetic disease. The shape of the face is affected in 30-40% of known genetic syndromes. Here, we determine whether syndromes can be diagnosed from 3D images of human faces.
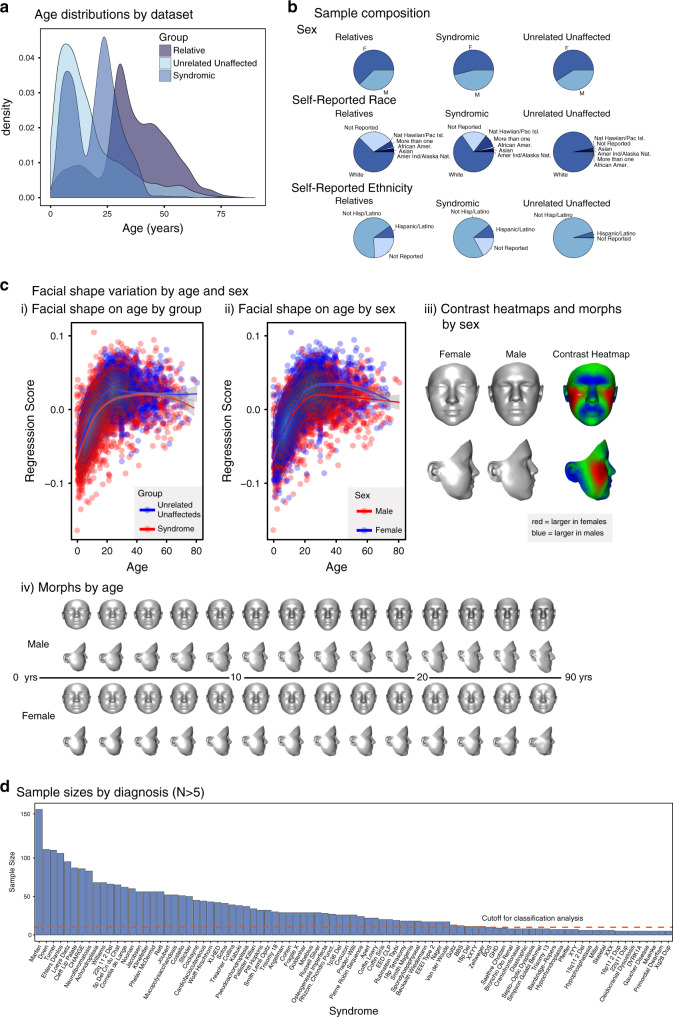
Methods: We analyzed variation in three-dimensional (3D) facial images of 7057 subjects: 3327 with 396 different syndromes, 727 of their relatives, and 3003 unrelated, unaffected subjects. We developed and tested machine learning and parametric approaches to automated syndrome diagnosis using 3D facial images.
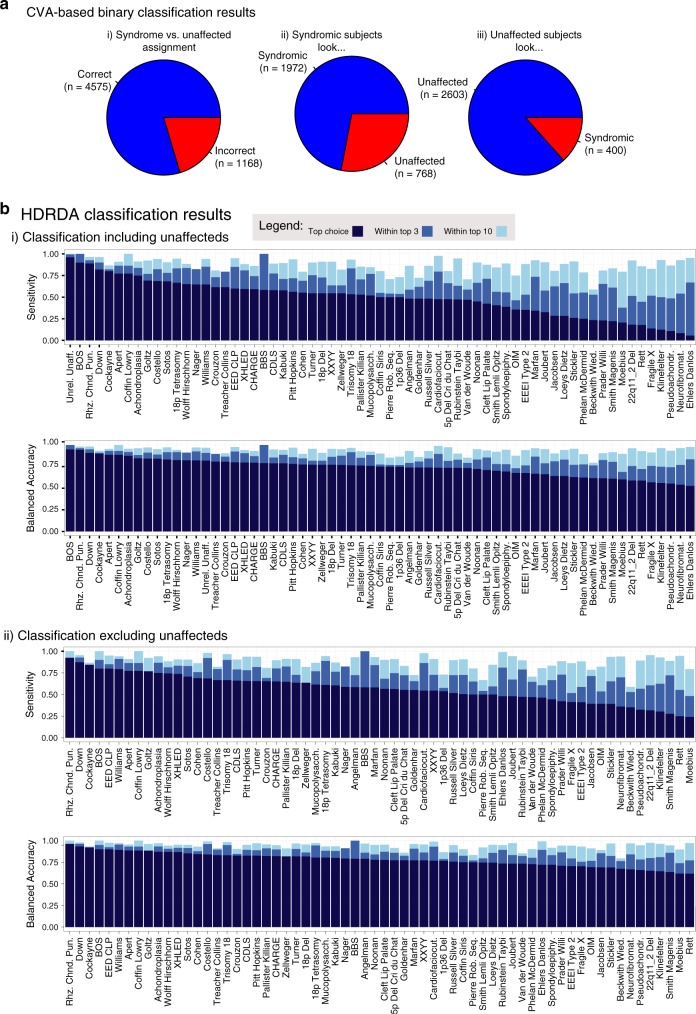
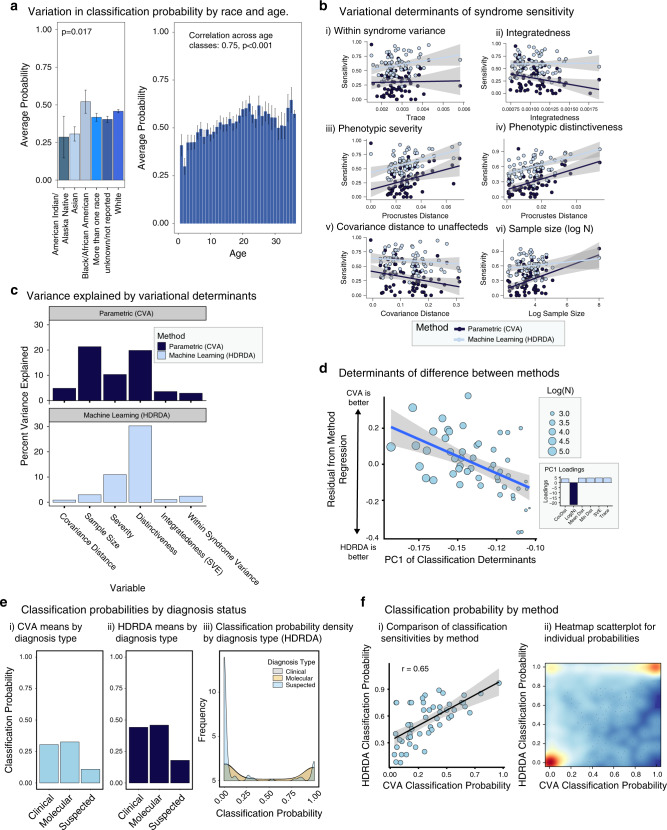
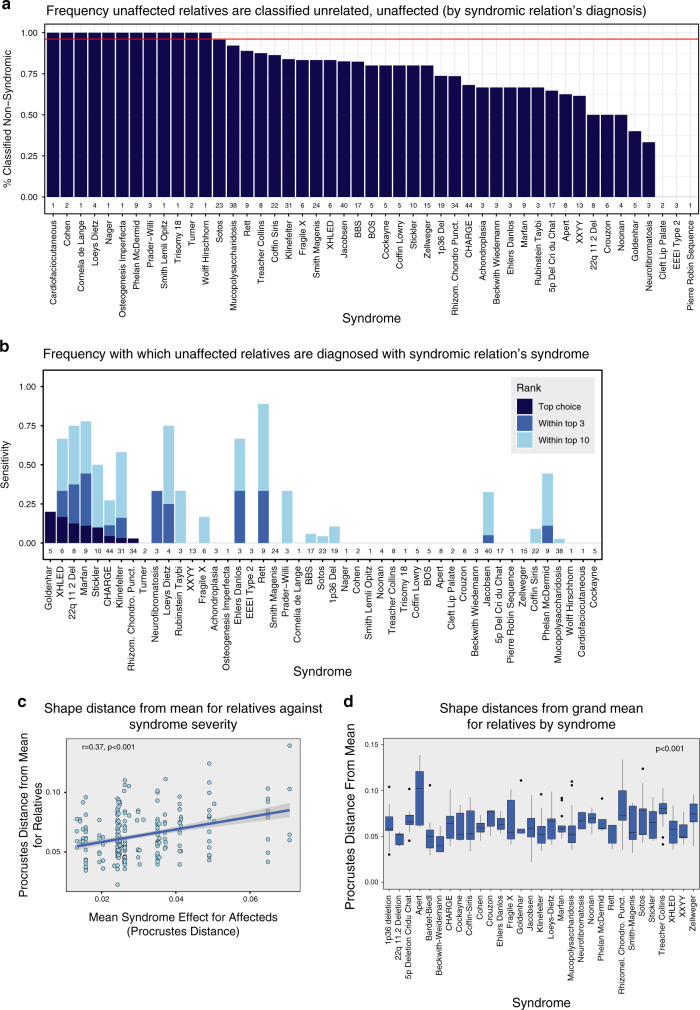
Results: Unrelated, unaffected subjects were correctly classified with 96% accuracy. Considering both syndromic and unrelated, unaffected subjects together, balanced accuracy was 73% and mean sensitivity 49%. Excluding unrelated, unaffected subjects substantially improved both balanced accuracy (78.1%) and sensitivity (56.9%) of syndrome diagnosis. The best predictors of classification accuracy were phenotypic severity and facial distinctiveness of syndromes. Surprisingly, unaffected relatives of syndromic subjects were frequently classified as syndromic, often to the syndrome of their affected relative.
Conclusion: Deep phenotyping by quantitative 3D facial imaging has considerable potential to facilitate syndrome diagnosis. Furthermore, 3D facial imaging of "unaffected" relatives may identify unrecognized cases or may reveal novel examples of semidominant inheritance.
Keywords: deep phenotyping; diagnosis; facial imaging; morphometrics; syndromes.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures