

Prognostic Value of Modified IHC4 Score in Patients with Estrogen Receptor-Positive Metastatic Breast Cancer
- PMID: 32476192
- PMCID: PMC7418366
- DOI: 10.1634/theoncologist.2019-1006
Prognostic Value of Modified IHC4 Score in Patients with Estrogen Receptor-Positive Metastatic Breast Cancer
Abstract
Background: This study aimed to investigate whether an immunohistochemical prognostic model (IHC4 score) can predict the prognosis and the chemotherapy benefit in patients with estrogen receptor-positive (ER+)/human epidermal growth receptor 2-negative (HER2-) metastatic breast cancer (MBC).
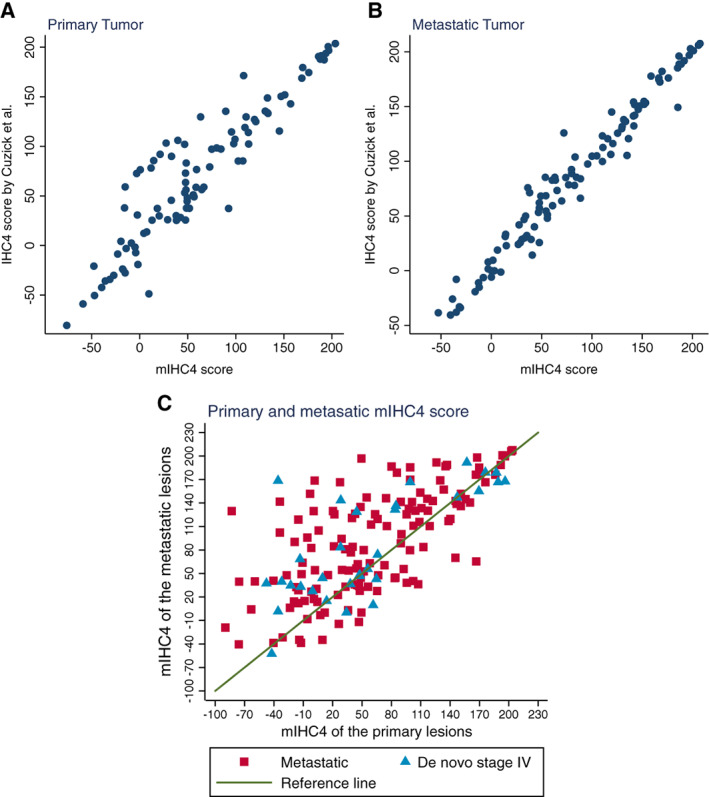
Materials and methods: We developed a method to calculate the modified IHC4 (mIHC4) scores based on routine pathological reports and compared them with the original IHC4 scores that were much more difficult to calculate. Univariate and multivariate analyses were used to study the prognostic factors of progression-free survival (PFS) and overall survival (OS). The predictive value of mIHC4 score was also investigated.
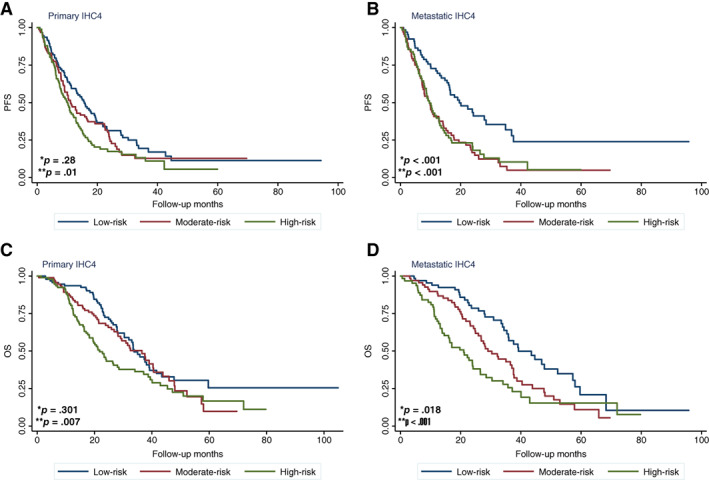
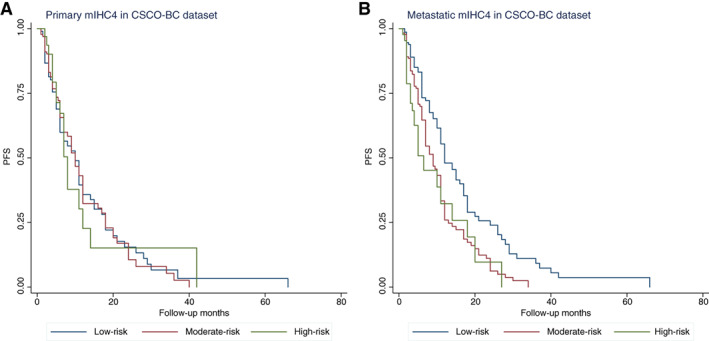
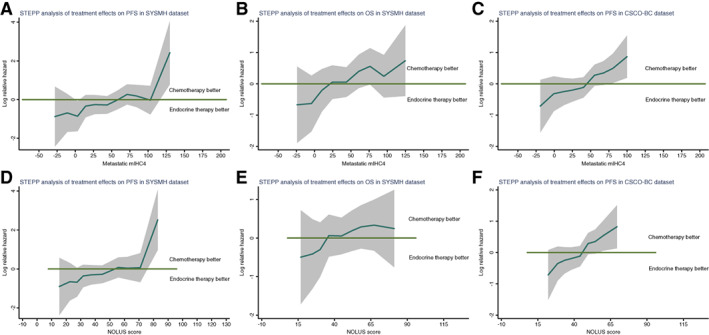
Results: The Sun Yat-sen Memorial Hospital data set included 315 patients with newly diagnosed ER+ MBC with a median follow-up of 25.6 months. Univariate and multivariate analysis showed that higher mIHC4 scores in metastatic lesions, but not the ones in primary tumors, were significantly associated with worse PFS and OS. The prognostic value of mIHC4 scores for PFS was validated using an independent Chinese Society of Clinical Oncology- Breast Cancer (CSCO-BC) data set. More importantly, subpopulation treatment effect pattern plot analysis showed that first-line endocrine therapy achieved better PFS and OS than chemotherapy in low-risk patients with ER+/HER2- MBC, whereas first-line chemotherapy was associated with improved PFS and OS compared with endocrine therapy in high-risk ones. The predictive value of mIHC4 score for PFS in selecting first-line endocrine therapy versus chemotherapy was also confirmed in the CSCO-BC data set.
Conclusion: mIHC4 scores in metastatic lesions are prognostic for the PFS and OS in patients with ER+ MBC. Low or high mIHC4 score may indicate the survival benefit in choosing first-line endocrine therapy or chemotherapy in patients with ER+/HER2- MBC, respectively.
Implications for practice: The modified IHC4 (mIHC4) score is easy to implement and able to predict patients with advanced and/or metastatic breast cancer. In addition, with the help of the mIHC4 score, physicians might be able to recommend chemotherapy or endocrine therapy as the first-line treatment for patients with high and low risk as predicted by the mIHC4 score.
Keywords: Chemotherapy; Endocrine therapy; IHC4; Metastatic breast cancer.
© 2020 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
References
-
- World Health Organization . Globocan 2018: Estimated cancer incidence, mortality and prevalence worldwide in 2018. Available at http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx. Accessed August 2019.
-
- Cardoso F, Harbeck N, Fallowfield L et al. Locally recurrent or metastatic breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow‐up. Ann Oncol 2012;23(suppl 7):vii11–vii19. - PubMed
-
- Chia SK, Speers CH, D'Yachkova Y et al. The impact of new chemotherapeutic and hormone agents on survival in a population‐based cohort of women with metastatic breast cancer. Cancer 2007;110:973–979. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
