

Complete Revascularization by Percutaneous Coronary Intervention for Patients With ST-Segment-Elevation Myocardial Infarction and Multivessel Coronary Artery Disease: An Updated Meta-Analysis of Randomized Trials
- PMID: 32476540
- PMCID: PMC7429036
- DOI: 10.1161/JAHA.119.015263
Complete Revascularization by Percutaneous Coronary Intervention for Patients With ST-Segment-Elevation Myocardial Infarction and Multivessel Coronary Artery Disease: An Updated Meta-Analysis of Randomized Trials
Abstract
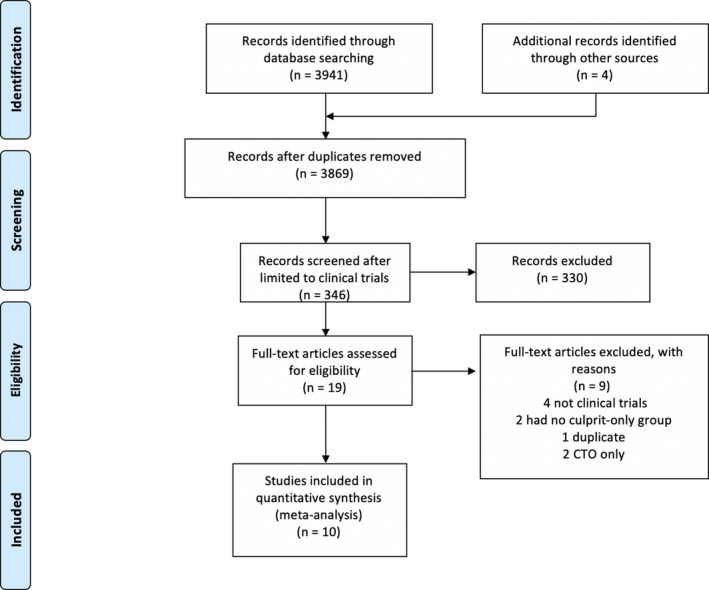
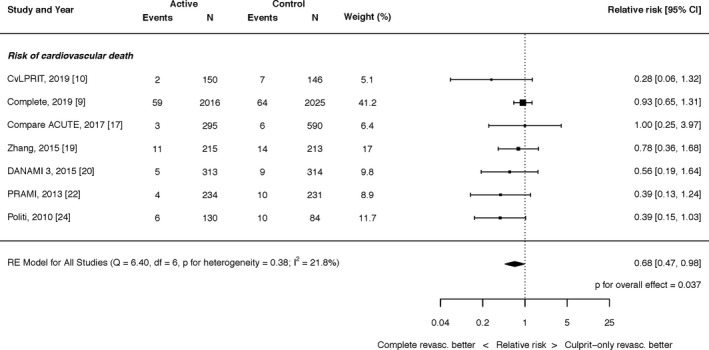
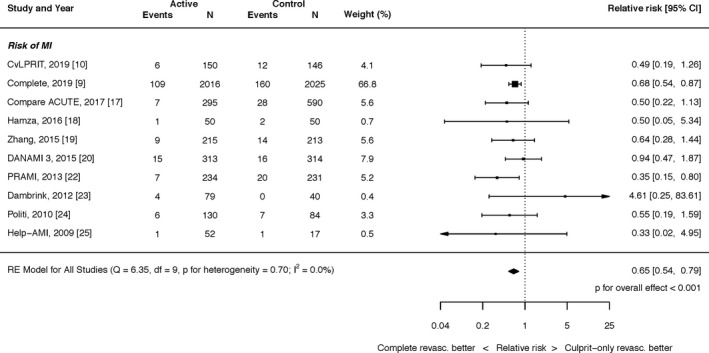
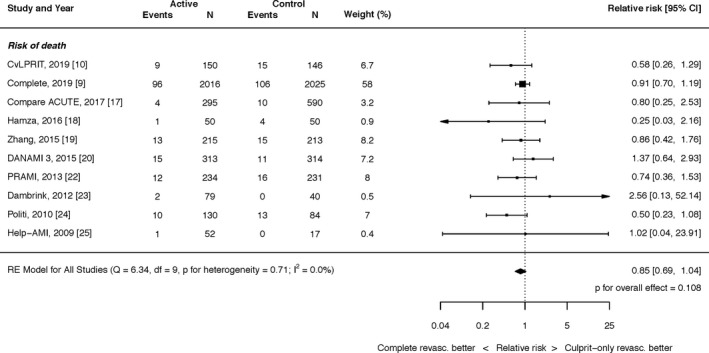
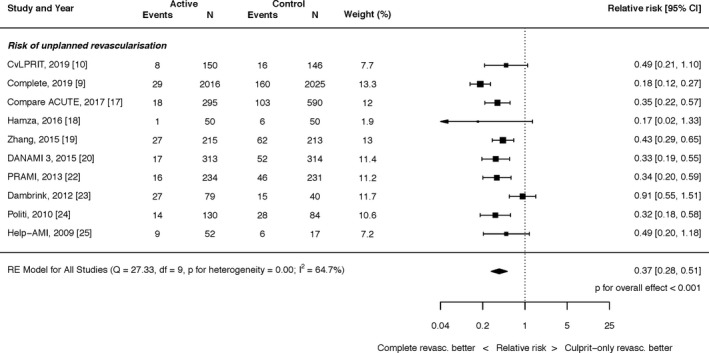
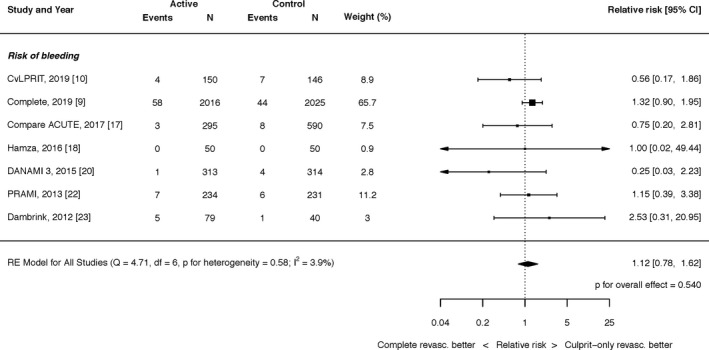
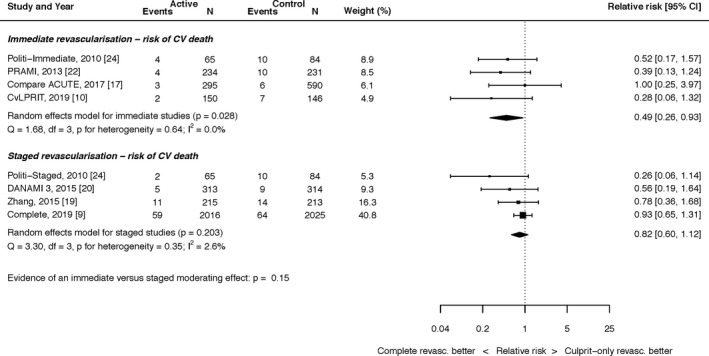
Background For patients with ST-segment-elevation myocardial infarction (STEMI) and multivessel coronary artery disease, the optimal treatment of the non-infarct-related artery has been controversial. This up-to-date meta-analysis focusing on individual clinical end points was performed to further evaluate the benefit of complete revascularization with percutaneous coronary intervention for patients with STEMI and multivessel coronary artery disease. Methods and Results We systematically identified all randomized trials comparing complete revascularization with percutaneous coronary intervention to culprit-only revascularization for multivessel disease in STEMI and performed a random-effects meta-analysis. The primary efficacy end point was cardiovascular death analyzed on an intention-to-treat basis. Secondary end points included all-cause mortality, myocardial infarction, and unplanned revascularization. Ten studies (7542 patients) were included: 3664 patients were randomized to complete revascularization and 3878 to culprit-only revascularization. Across all patients, complete revascularization was superior to culprit-only revascularization for reduction in the risk of cardiovascular death (relative risk [RR], 0.68; 95% CI, 0.47-0.98; P=0.037; I2=21.8%) and reduction in the risk of myocardial infarction (RR, 0.65; 95% CI, 0.54-0.79; P<0.0001; I2=0.0%). Complete revascularization also significantly reduced the risk of unplanned revascularization (RR, 0.37; 95% CI, 0.28-0.51; P<0.0001; I2=64.7%). The difference in all-cause mortality with percutaneous coronary intervention was not statistically significant (RR, 0.85; 95% CI, 0.69-1.04; P=0.108; I2=0.0%). Conclusions For patients with STEMI and multivessel disease, complete revascularization with percutaneous coronary intervention significantly improves hard clinical outcomes including cardiovascular death and myocardial infarction. These data have implications for clinical practice guidelines regarding recommendations for complete revascularization following STEMI.
Keywords: ST‐segment–elevation myocardial infarction; percutaneous coronary intervention; revascularization.
Figures
References
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. - PubMed
-
- Rasoul S, Ottervanger JP, de Boer M‐J, Dambrink J‐HE, Hoorntje JCA, Marcel Gosselink AT, Zijlstra F, Suryapranata H, van ‘t Hof AWJ; Zwolle Myocardial Infarction Study Group . Predictors of 30‐day and 1‐year mortality after primary percutaneous coronary intervention for ST‐elevation myocardial infarction. Coron Artery Dis. 2009;20:415–421. - PubMed
-
- Sorajja P, Gersh BJ, Cox DA, McLaughlin MG, Zimetbaum P, Costantini C, Stuckey T, Tcheng JE, Mehran R, Lansky AJ, et al. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur Heart J. 2007;28:1709–1716. - PubMed
-
- Authors/Task Force members , Windecker S, Kolh P, Alfonso F, Collet J‐P, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Jüni P, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio‐Thoracic Surgery (EACTS). Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35:2541–2619. - PubMed
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, et al.; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines . 2013 ACCF/AHA guideline for the management of ST‐elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425. - PubMed
