

Procedural Volume and Outcomes After Primary Percutaneous Coronary Intervention for ST-Segment-Elevation Myocardial Infarction in Kerala, India: Report of the Cardiological Society of India-Kerala Primary Percutaneous Coronary Intervention Registry
- PMID: 32476563
- PMCID: PMC7429028
- DOI: 10.1161/JAHA.119.014968
Procedural Volume and Outcomes After Primary Percutaneous Coronary Intervention for ST-Segment-Elevation Myocardial Infarction in Kerala, India: Report of the Cardiological Society of India-Kerala Primary Percutaneous Coronary Intervention Registry
Abstract
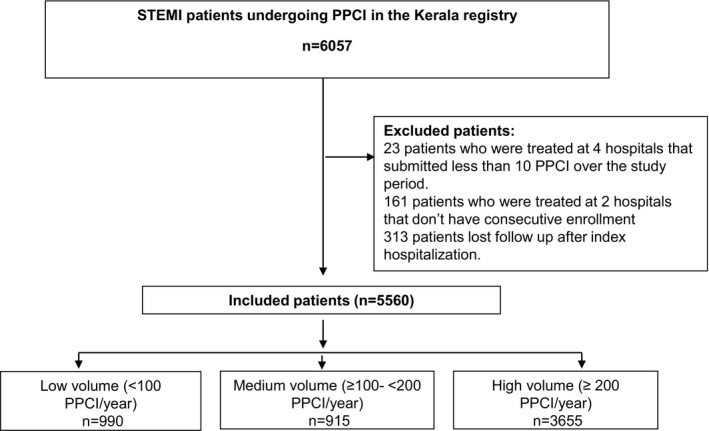
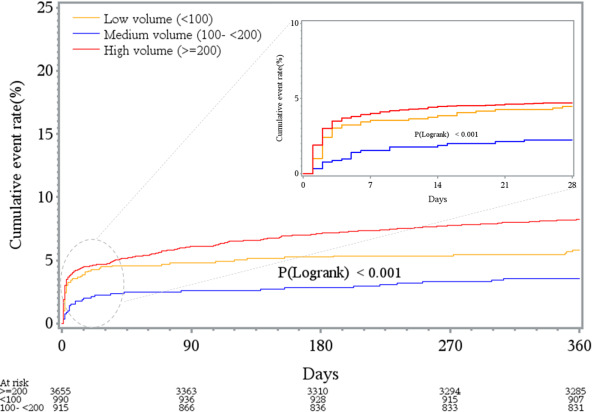
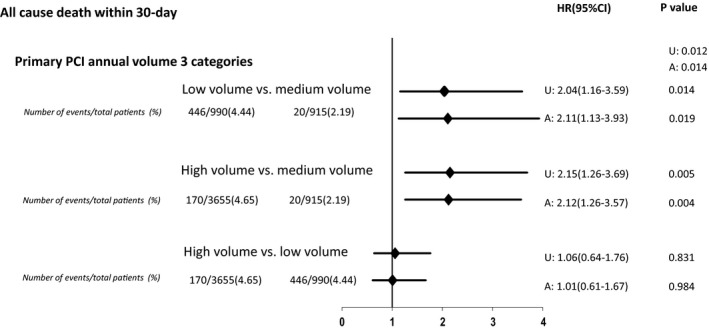
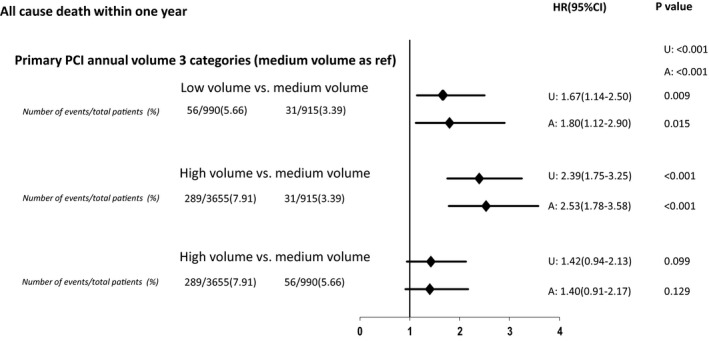
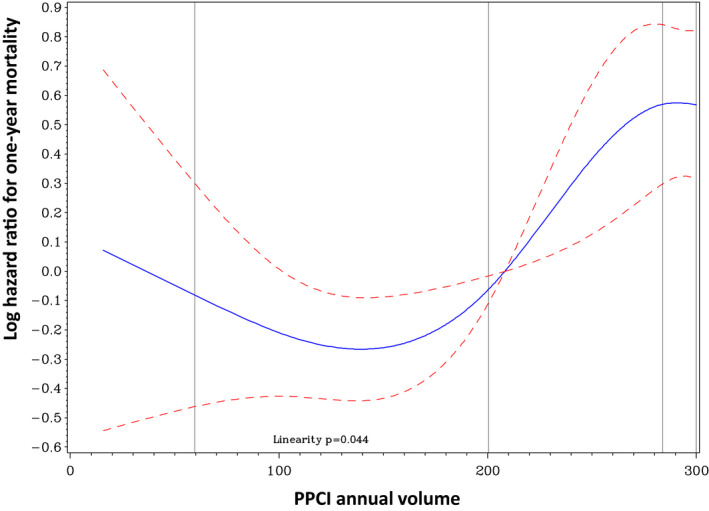
Background There are limited data to inform policy mandating primary percutaneous coronary intervention (PPCI) volume benchmarks for catheterization laboratories in low- and middle-income countries. Methods and Results This prospective state-wide registry included ST-segment-elevation myocardial infarction patients with symptoms of <12 hours, or with ongoing ischemia at 12 to 24 hours, reperfused with PPCI. From June 2013 to March 2016, we recruited 5560 consecutive patients. We categorized hospitals on the basis of annual PPCI volumes into low, medium, and high volume (<100, 100-199, and ≥200 PPCIs per year, respectively). Kaplan-Meier curves and Cox regression models were used to examine the association between PPCI volume and 1-year mortality. Among 42 recruiting hospitals, there were 24 (57.2%) low-volume, 8 (19%) medium-volume, and 10 (23.8%) high-volume hospitals. The median (25th-75th percentile) TIMI (Thrombolysis in Myocardial Infarction) ST-segment-elevation myocardial infarction risk score was 3 (2-5). Cardiac arrest before admission occurred in 4.2%, 2.1%, and 2.9% of cases at low-, medium-, and high-volume hospitals, respectively (P=0.02). Total ischemic time differed significantly among low-volume (median [25th-75th percentile], 3.5 [2.4-5.5] hours), medium-volume (median, 3.8 [25th-75th percentile, 2.58-6.05] hours), and high-volume hospitals (median, 4.16 [25th-75th percentile 2.8-6.3] hours) (P=0.01). Vascular access was radial in 61.5%, 71.3%, and 63.2% of cases at low-, medium-, and high-volume hospitals, respectively (P=0.01). The observed 1-year mortality rate was 6.5%, 3.4%, and 8.6% at low-, medium- and high-volume hospitals, respectively (P<0.01), and the difference did not attenuate after multivariate adjustment (low versus medium: hazard ratio [95% CI], 1.80 [1.12-2.90]; high versus medium: hazard ratio [95% CI], 2.53 [1.78-3.58]) (P<0.01). Conclusions Low- and middle-income countries, like India, may have a nonlinear relationship between institutional PPCI volume and outcomes, partly driven by procedural variations and inequalities in access to care.
Keywords: ST‐segment–elevation myocardial infarction; percutaneous coronary intervention; stents.
Figures
References
-
- Prabhakaran D, Jeemon P, Roy A. Cardiovascular diseases in India: current epidemiology and future directions. Circulation. 2016;133:1605–1620. - PubMed
-
- Mohanan PP, Mathew R, Harikrishnan S, Krishnan MN, Zachariah G, Joseph J, Eapen K, Abraham M, Menon J, Thomas M, et al. Presentation, management, and outcomes of 25 748 acute coronary syndrome admissions in Kerala, India: results from the Kerala ACS Registry. Eur Heart J. 2013;34:121–129. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
