

Impact of a standardized reporting format on the quality of MRI reports for rectal cancer staging
- PMID: 32476744
- PMCID: PMC7240900
- DOI: 10.4103/ijri.IJRI_308_19
Impact of a standardized reporting format on the quality of MRI reports for rectal cancer staging
Abstract
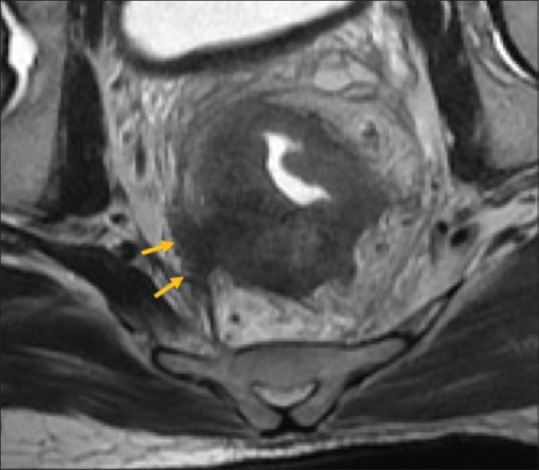
Background and aims: Besides providing a surgical roadmap, rectal MRI plays a major role in treatment planning. We recently started using a structured template for reporting rectal cancer via MRI. We study the impact of using this template at our hospital in terms of number of essential imaging parameters described in the reports as compared to the pre-template free-text reports.
Methods: A structured rectal MRI reporting template was created in consensus with members of the colorectal tumour board and was introduced in the department, which included 14 essential parameters to be mentioned in the reports. We conducted a retrospective analysis of rectal MRI reports of 100 cases with histologically proven rectal cancer, comprising 50 consecutive free-text reports before the template was introduced and 50 consecutive structured reports after its introduction, checking for the presence or absence of inclusion of the 14 parameters. An anonymous online feedback survey was conducted as well after the introduction of the template for the members of the colorectal tumour board.
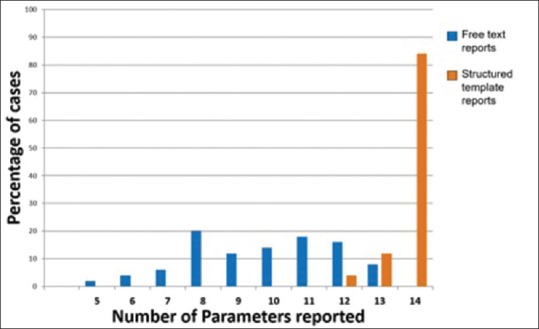
Results: Overall, the total number of parameters reported increased from a median value of 10 (range 6-13) to 14 (range 12-14). The common unreported parameters prior to template introduction included T staging, presence or absence of restricted diffusion, anterior peritoneal reflection (APR) involvement, and presence or absence of extramural vascular invasion; these were reported in 16%, 22%, 30% and 50% respectively. These improved to 98-100% reporting after template introduction. Maximum improvement was in T staging (16% to 98%) (P < 0.0001), restricted diffusion on DWI (from 22% to 100%) (P < 0.0001) and APR involvement (from 30% to 100%) (P < 0.0001). The most common unreported parameter after template introduction was the "tumoral T2 signal intensity" (unreported in 4% cases). The results of the survey were as follows: 100% felt a decreased need to talk to the radiologist to clarify the report, 81.8% felt an improvement in the quality of reporting as compared to free style reports, and 91% felt that the new template is easier to interpret.
Conclusion: The introduction of a structured template for rectal cancer significantly improved the quality of rectal MRI reports, along with the satisfaction of referring providers.
Keywords: Cancer; rectal; reporting; structured; template.
Copyright: © 2020 Indian Journal of Radiology and Imaging.
Conflict of interest statement
There are no conflicts of interest.
Figures






References
-
- Tersteeg JJC, Gobardhan PD, Crolla RMPH, Kint PA, Niers-Stobbe I, Boonman–de Winter LJM, et al. Improving the quality of MRI reports of preoperative patients with rectal cancer: Effect of national guidelines and structured reporting. Am J Roentgenol. 2018;1:1240–4. - PubMed
-
- Sahni VA, Silveira PC, Sainani NI, Khorasani R. Impact of a structured report template on the quality of MRI reports for rectal cancer staging. Am J Roentgenol. 2015;205:584–8. - PubMed
-
- Nörenberg D, Sommer WH, Thasler W, D'haese J, Rentsch M, Kolben T, et al. Structured reporting of rectal magnetic resonance imaging in suspected primary rectal cancer: Potential benefits for surgical planning and interdisciplinary communication. Invest Radiol. 2017;52:232–9. - PubMed
-
- Gollub MJ, Arya S, Beets-Tan RG, Gonen M, Jhaveri K, Kassam Z, et al. Use of magnetic resonance imaging in rectal cancer patients: Society of Abdominal Radiology (SAR) rectal cancer disease-focused panel (DFP) recommendations 2017. Abdom Radiol. 2018;43:2893–902. - PubMed
-
- Beets-Tan RG, Lambregts DM, Maas M, Bipat S, Barbaro B, Curvo-Semedo L, et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2018;28:1465–75. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous