

Necrotising sarcoid granulomatosis. A rare granulomatous disease
- PMID: 32476929
- PMCID: PMC7170123
- DOI: 10.36141/svdld.v35i4.7047
Necrotising sarcoid granulomatosis. A rare granulomatous disease
Abstract
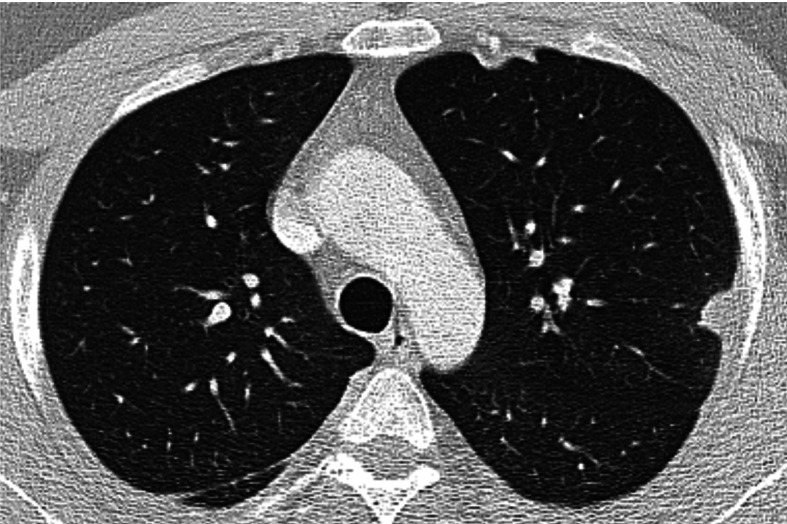
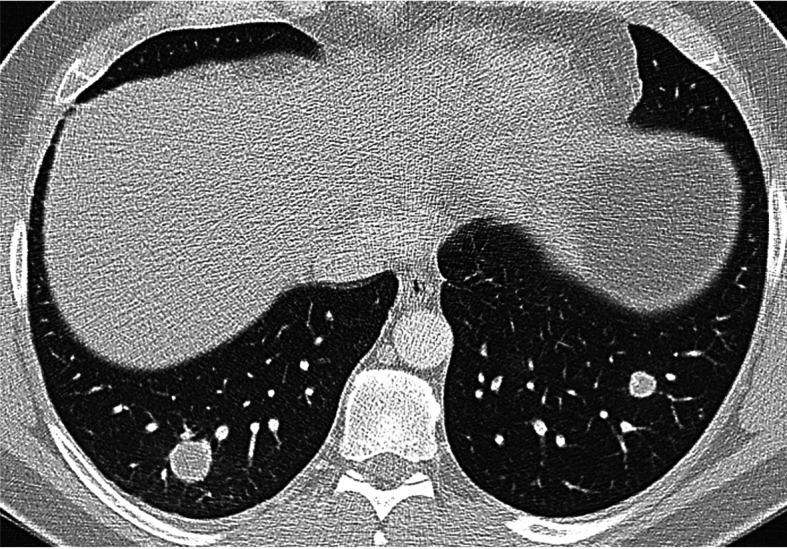
Introduction: Necrotizing sarcoid granulomatosis (NSG) is a very rare disease of unknown etiology characterized by sarcoid-like granulomas, vasculitis and necrosis in pulmonary and extrapulmonary localizations. Case report: We describe a case of a 34-year-old Caucasian male with fever, pleural pain, and nodular pulmonary opacities on chest radiograph. Histological examination of the lung tissue confirmed NSG. Diagnostically, infectious causes, vasculitis, and malignancy were excluded. A tendency to partial regression was observed, without the need for corticosteroid treatment. Conclusion: NSG is a rare disease which must be distinguished from other systemic diseases including vasculitides. The key to diagnosis, emphasized in our paper, is the histopathological finding. The course of NSG is similar to sarcoidosis. Corticosteroids are considered the treatment of choice, but the disease exhibits a tendency towards spontaneous regression. (Sarcoidosis Vasc Diffuse Lung Dis 2018; 35: 395-398).
Keywords: differential diagnosis; histopathological diagnosis; necrotising sarcoid granulomatosis.
Copyright: © 2018 SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES.
Figures



References
-
- Liebow AA. The J. Burns Amberson lecture – pulmonary angiitis and granulomatosis. Am Rev Respir Dis. 1973;108(1):1–18. - PubMed
-
- Churg A. Pulmonary angiitis and granulomatosis revisited. Hum Pathol. 1983;14(10):868–883. - PubMed
-
- Churg A, Carrington GB, Gupta R. Necrotizing sarcoid granulomatosis. Chest. 1979;76(4):406–413. - PubMed
-
- Quaden C, Tillie-Leblond I, Delobbe A, et al. Necrotising sarcoid granulomatosis: clinical, functional, endoscopical and radiographical evaluations. Eur Respir J. 2005;26(5):778–85. - PubMed
-
- Bouman KP, Slabbynck H, Cuykens JJ, Galdermans D, Coolen D, Kock M. Necrotising sarcoid granulomatosis with uveitis: a variant of sarcoidosis. Acta Clin Belg. 1997;52(6):367–370. - PubMed
Publication types
LinkOut - more resources
Full Text Sources