

Changes in Myocardial Microstructure and Mechanics With Progressive Left Ventricular Pressure Overload
- PMID: 32478208
- PMCID: PMC7251228
- DOI: 10.1016/j.jacbts.2020.02.007
Changes in Myocardial Microstructure and Mechanics With Progressive Left Ventricular Pressure Overload
Abstract
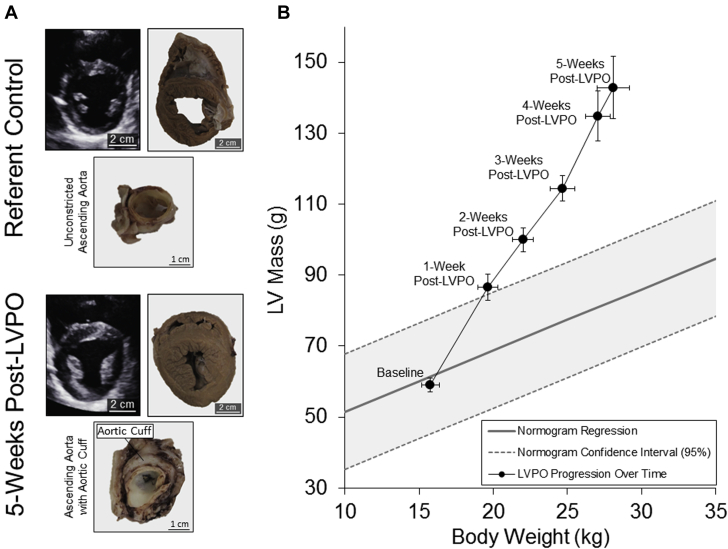
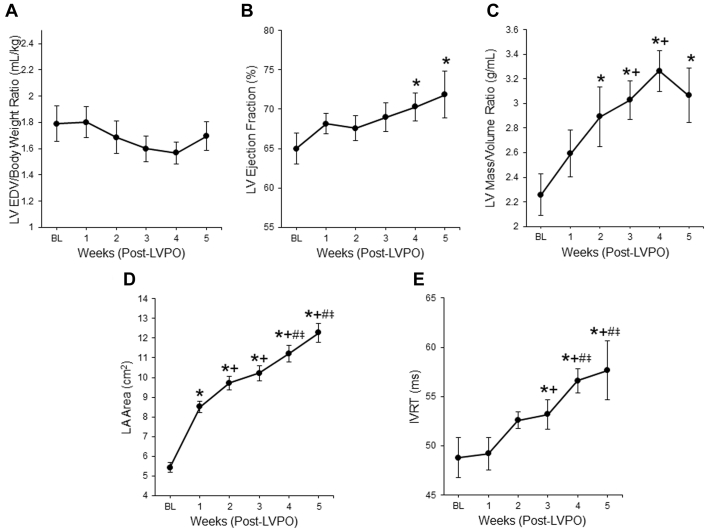
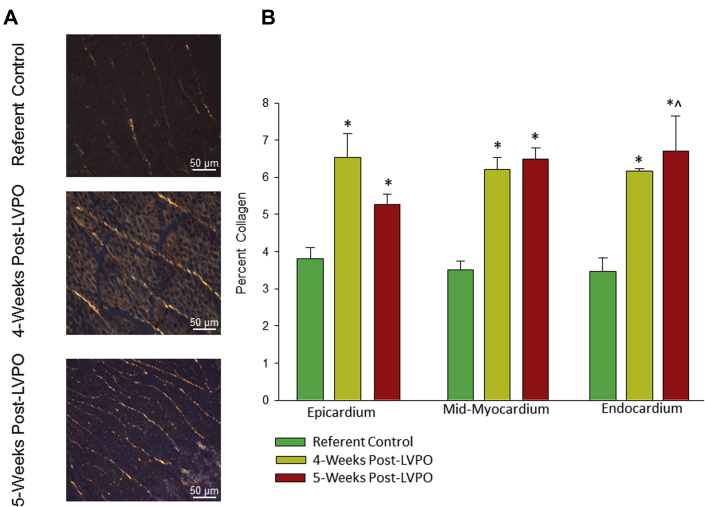
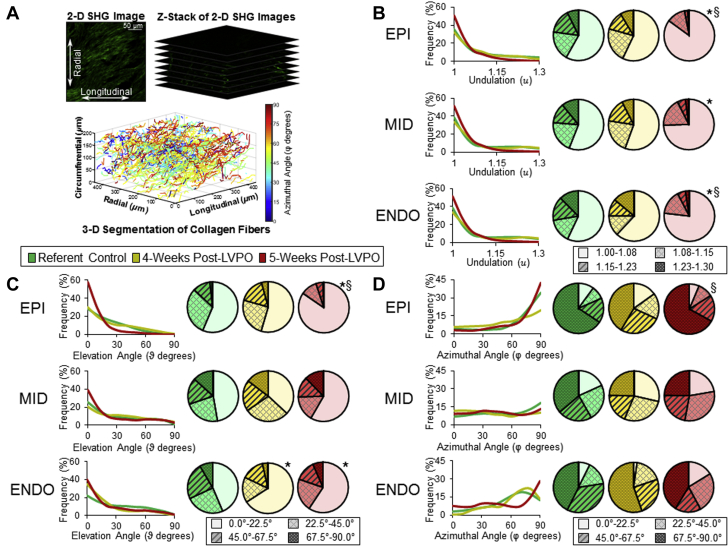
This study assessed the regional changes in myocardial geometry, microstructure, mechanical behavior, and properties that occur in response to progressive left ventricular pressure overload (LVPO) in a large animal model. Using an index of local biomechanical function at early onset of LVPO allowed for prediction of the magnitude of left ventricular chamber stiffness (Kc) and left atrial area at LVPO late timepoints. Our study found that LV myocardial collagen content alone was insufficient to identify mechanisms for LV myocardial stiffness with progression to heart failure with preserved ejection fraction (HFpEF). Serial assessment of regional biomechanical function might hold value in monitoring the natural history and progression of HFpEF, which would allow evaluation of novel therapeutic approaches.
Keywords: Ct, cycle time; EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IVRT, isovolumic relaxation time; LA, left atrial; LV, left ventricular; LVPO, left ventricular pressure overload; NT-proBNP, N-terminal pro-brain natriuretic peptide; PCR, polymerase chain reaction; PRSW, pre-load recruitable stroke work; SHG, second harmonic generation; STE, speckle tracking echocardiography; echocardiography; heart failure; pressure overload; qPCR, quantitative real-time PCR.
© 2020 Published by Elsevier on behalf of the American College of Cardiology Foundation.
Figures





Comment in
-
Interstitial Fibrosis and Diastolic Dysfunction in Aortic Stenosis.JACC Basic Transl Sci. 2020 May 25;5(5):481-483. doi: 10.1016/j.jacbts.2020.03.014. eCollection 2020 May. JACC Basic Transl Sci. 2020. PMID: 32479575 Free PMC article.
References
-
- Bursi F., Weston S.A., Redfield M.M. Systolic and diastolic heart failure in the community. JAMA. 2006;296:2209–2216. - PubMed
-
- Bronzwaer J.G.F., Paulus W.J. Diastolic and systolic heart failure: different stages or distinct phenotypes of the heart failure syndrome? Curr Heart Fail Rep. 2009;6:281–286. - PubMed
-
- Komajda M., Carson P.E., Hetzel S. Factors associated with outcome in heart failure with preserved ejection fraction: findings from the Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-PRESERVE) Circ Heart Fail. 2011;4:27–35. - PubMed
-
- Zile M.R., Gaasch W.H., Anand I.S. Mode of death in patients with heart failure and a preserved ejection fraction: results from the irbesartan in heart failure with preserved ejection fraction study (I-Preserve) Trial. Circulation. 2010;121:1393–1405. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
