

Brown tumor of the iliac crest initially misdiagnosed as a giant cell tumor of the bone
- PMID: 32478667
- PMCID: PMC7219131
- DOI: 10.1530/EDM-20-0029
Brown tumor of the iliac crest initially misdiagnosed as a giant cell tumor of the bone
Abstract
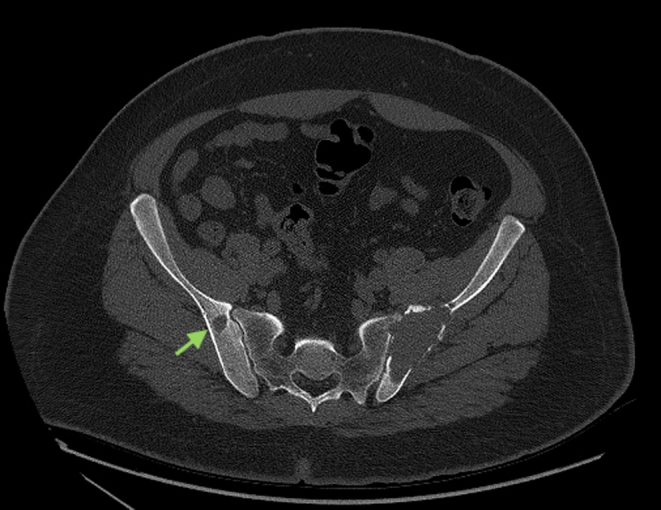
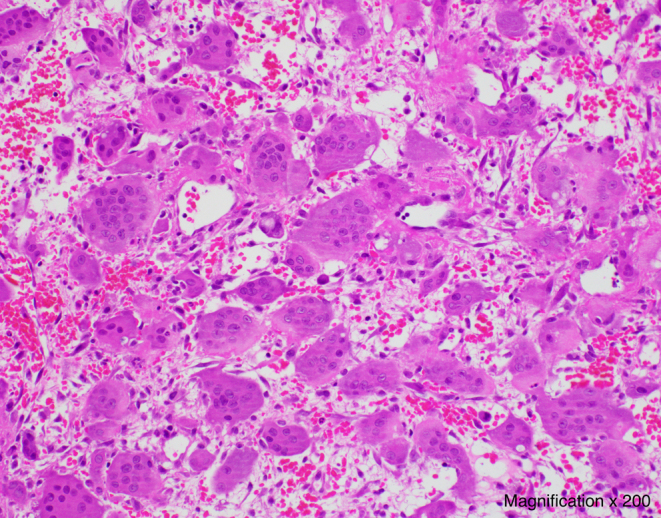
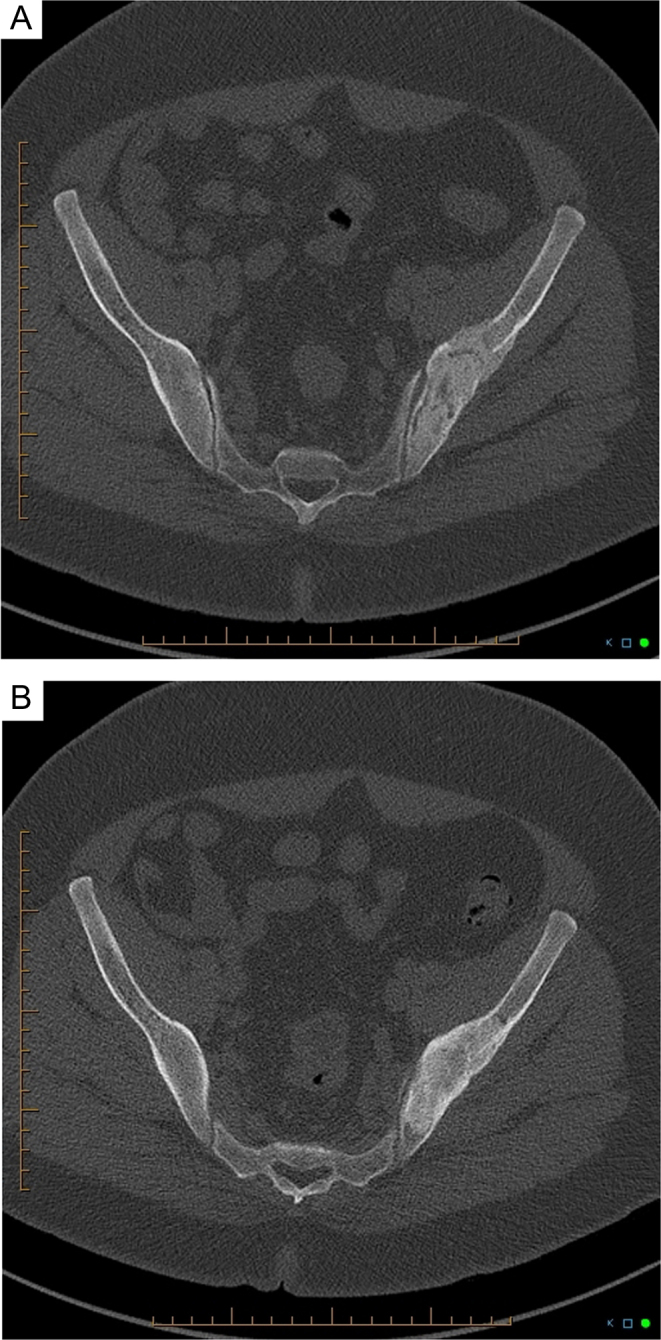
Summary: Brown tumors (BTs) are expansile osteolytic lesions complicating severe primary hyperparathyroidism (PHPT). Clinical, radiological and histological features of BTs share many similarities with other giant cell-containing lesions of the bone, which can make their diagnosis challenging. We report the case of a 32-year-old man in whom an aggressive osteolytic lesion of the iliac crest was initially diagnosed as a giant cell tumor by biopsy. The patient was scheduled for surgical curettage, with a course of neoadjuvant denosumab. Routine biochemical workup prior to denosumab administration incidentally revealed high serum calcium levels. The patient was diagnosed with PHPT and a parathyroid adenoma was identified. In light of these findings, histological slices of the iliac lesion were reviewed and diagnosis of a BT was confirmed. Follow-up CT-scans performed 2 and 7 months after parathyroidectomy showed regression and re-ossification of the bone lesion. The aim of this case report is to underline the importance of distinguishing BTs from other giant cell-containing lesions of the bone and to highlight the relevance of measuring serum calcium as part of the initial evaluation of osteolytic bone lesions. This can have a major impact on patients' management and can prevent unnecessary invasive surgical interventions.
Learning points: Although rare, brown tumors should always be considered in the differential diagnosis of osteolytic giant cell-containing bone lesions. Among giant cell-containing lesions of the bone, the main differential diagnoses of brown tumors are giant cell tumors and aneurysmal bone cysts. Clinical, radiological and histological characteristics can be non-discriminating between brown tumors and giant cell tumors. One of the best ways to distinguish these two diagnoses appears to be through biochemical workup. Differentiating brown tumors from giant cell tumors and aneurysmal bone cysts is crucial in order to ensure better patient care and prevent unnecessary morbid surgical interventions.
Keywords: 2020; 25-hydroxyvitamin-D3; Adult; April; Bone; Bone biopsy; Bone lesions; Brown tumour; CT scan; Calcitriol; Calcium (serum); Calcium carbonate; Canada; Cholecalciferol; Denosumab; Error in diagnosis/pitfalls and caveats; Histopathology; Hypercalcaemia; Hyperparathyroidism (primary); MRI; Male; Other; PTH; Parathyroid; Parathyroid adenoma; Parathyroidectomy; Pathology; Phosphate (serum); Radiology/Rheumatology; Sestamibi scan; Surgery; X-ray.
Figures

References
-
- Khan AA, Hanley DA, Rizzoli R, Bollerslev J, Young JE, Rejnmark L, Thakker R, D’Amour P, Paul T, Van Uum S, et al Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and International Consensus. Osteoporosis International 2017. 28 1–19. (10.1007/s00198-016-3716-2) - DOI - PMC - PubMed
-
- Rosenberg AE, Nielsen GP. Giant cell containing lesions of bone and their differential diagnosis. Current Diagnostic Pathology 2001. 7 235–246. (10.1054/cdip.2001.0080) - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
