

Effects of In-Person Navigation to Address Family Social Needs on Child Health Care Utilization: A Randomized Clinical Trial
- PMID: 32478849
- PMCID: PMC7265099
- DOI: 10.1001/jamanetworkopen.2020.6445
Effects of In-Person Navigation to Address Family Social Needs on Child Health Care Utilization: A Randomized Clinical Trial
Abstract
Importance: While many organizations endorse screening for social risk factors in clinical settings, few studies have examined the health and utilization effects of interventions to address social needs.
Objective: To compare the acute care utilization effects of a written resources handout vs an in-person navigation service intervention to address social needs.
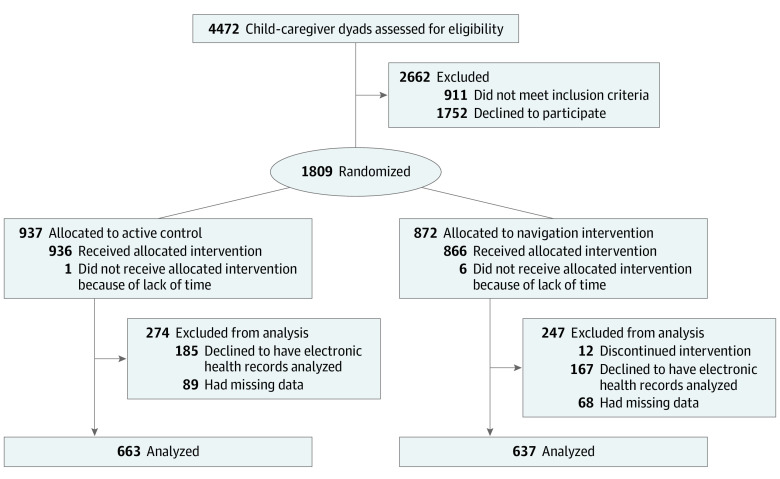
Design, settings, and participants: In this secondary analysis of a randomized clinical trial, 1809 adult caregivers of pediatric patients seen in primary and urgent care clinics of 2 safety-net hospitals in northern California were recruited between October 13, 2013, and August 27, 2015. Each participating family was randomly assigned to an in-person navigator intervention vs active control to address the family's social needs. Analyses were conducted between February 28, 2018, and September 25, 2019.
Interventions: Caregivers either received written information about relevant local resources related to social needs (active control) or met with a patient navigator focused on helping them resolve social needs (navigator intervention). After an initial in-person visit, navigation services included telephone, email, and/or in-person follow-up for up to 3 months.
Main outcome and measures: Child emergency department visit or hospitalization within 12 months of study enrollment.
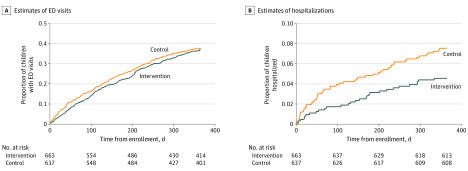
Results: Among the 1300 caregivers enrolled in the study without missing follow-up data, most spoke English (878 [67.5%]) and were women (1127 [86.7%]), with a mean (SD) age of 33.0 (9.33) years. Most children were aged 0 to 5 years (779 of 1300 [59.9%]), 723 children (55.6%) had Hispanic ethnicity, and 462 children (35.5%) were in excellent health; 840 families (64.6%) were recruited from urgent care. In total, 637 families (49.0%) were randomized to the in-person navigator group and 663 (51.0%) to the active control group. There was no difference in risk of an emergency department visit between the 2 groups. Children enrolled in the in-person navigator group had a decreased risk of hospitalization within 12 months (hazard ratio, 0.59; 05% CI, 0.38-0.94; P = .03), making them 69% less likely to be hospitalized.
Conclusions and relevance: In this randomized clinical trial evaluating heath care utilization effects of programs designed to address social needs among families, children enrolled in the navigation group were significantly less likely to be hospitalized after the intervention but equally likely to have an emergency department visit. These findings strengthen our understanding of the effects of addressing social needs in clinical settings as part of a comprehensive strategy to improve health and reduce health care utilization.
Trial registration: ClinicalTrials.gov Identifier: NCT01939704.
Conflict of interest statement
Figures
Comment in
-
Improving Child Health Care Outcomes Through Social Needs Intervention-A Signal.JAMA Netw Open. 2020 Jun 1;3(6):e206456. doi: 10.1001/jamanetworkopen.2020.6456. JAMA Netw Open. 2020. PMID: 32478844 No abstract available.
References
-
- Beck AF, Cohen AJ, Colvin JD, et al. . Perspectives from the Society for Pediatric Research: interventions targeting social needs in pediatric clinical care. Pediatr Res. 2018;84(1):10-21. - PubMed
-
- Crawford C. EveryONE Project unveils social determinants of health tools. Accessed March 22, 2018. https://www.aafp.org/news/health-of-the-public/20180109sdohtools.html
-
- Institute of Medicine Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2. National Academies Press; 2014. - PubMed
