

Impact of COVID-19 pandemic on ST-elevation myocardial infarction in a non-COVID-19 epicenter
- PMID: 32478961
- PMCID: PMC7300525
- DOI: 10.1002/ccd.28997
Impact of COVID-19 pandemic on ST-elevation myocardial infarction in a non-COVID-19 epicenter
Abstract
Objectives: We sought to study the impact of COVID-19 pandemic on the presentation delay, severity, patterns of care, and reasons for delay among patients with ST-elevation myocardial infarction (STEMI) in a non-hot-spot region.
Background: COVID-19 pandemic has significantly reduced the activations for STEMI in epicenters like Spain.
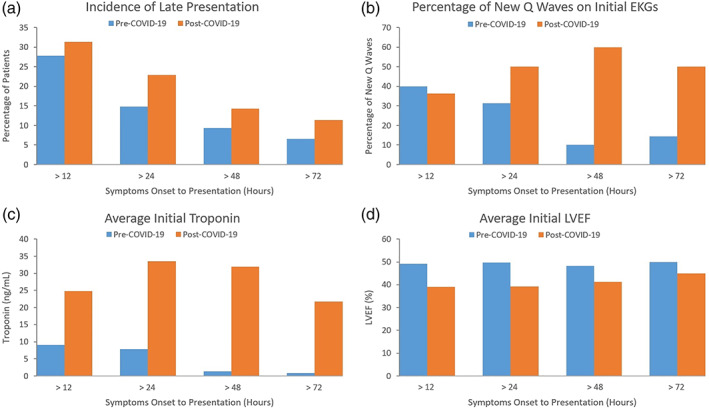
Methods: From January 1, 2020, to April 15, 2020, 143 STEMIs were identified across our integrated 18-hospital system. Pre- and post-COVID-19 cohorts were based on March 23rd, 2020, whenstay-at-home orders were initiated in Ohio. We used presenting heart rate, blood pressure, troponin, new Q-wave, and left ventricle ejection fraction (LVEF) to assess severity. Duration of intensive care unit stay, total length of stay, door-to-balloon (D2B) time, and radial versus femoral access were used to assess patterns of care.
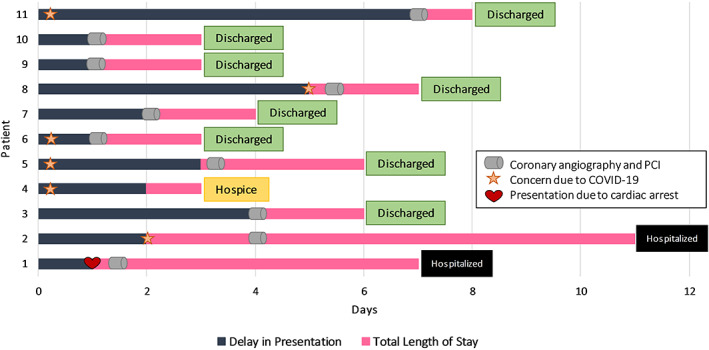
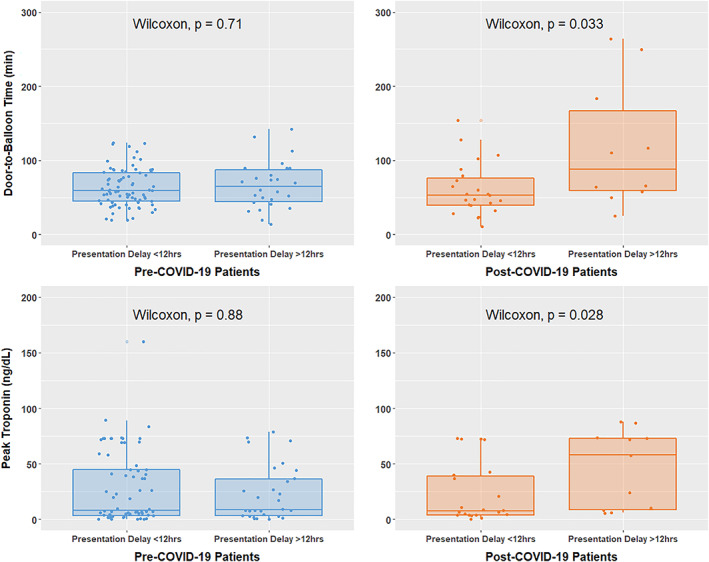
Results: Post-COVID-19 presentation was associated with a lower admission LVEF (45 vs. 50%, p = .015), new Q-wave, and higher initial troponin; however, these did not reach statistical significance. Among post-COVID-19 patients, those with >12-hr delay in presentation 31(%) had a longer average D2B time (88 vs. 53 min, p = .033) and higher peak troponin (58 vs. 8.5 ng/ml, p = .03). Of these, 27% avoided the hospital due to fear of COVID-19, 18% believed symptoms were COVID-19 related, and 9% did not want to burden the hospital during the pandemic.
Conclusions: COVID-19 has remarkably affected STEMI presentation and care. Patients' fear and confusion about symptoms are integral parts of this emerging public health crisis.
Keywords: coronavirus; delayed presentation; door-to-balloon; length of stay; troponin.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures
Comment in
-
Out-of-hospital cardiac arrest prognosis during the COVID-19 pandemic.Intern Emerg Med. 2020 Aug;15(5):875-877. doi: 10.1007/s11739-020-02428-7. Epub 2020 Jul 9. Intern Emerg Med. 2020. PMID: 32647947 Free PMC article. No abstract available.
References
-
- Mahmud E, Dauerman HL, Welt FG, et al. Management of Acute Myocardial Infarction during the COVID‐19 pandemic. Catheter Cardiovasc Interv. 2020;96(2):336‐345. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
