

Correlation of increased serum leucine-rich α2-glycoprotein levels with disease prognosis, progression, and activity of interstitial pneumonia in patients with dermatomyositis: A retrospective study
- PMID: 32479560
- PMCID: PMC7263588
- DOI: 10.1371/journal.pone.0234090
Correlation of increased serum leucine-rich α2-glycoprotein levels with disease prognosis, progression, and activity of interstitial pneumonia in patients with dermatomyositis: A retrospective study
Abstract
Objective: To investigate whether leucine-rich α2-glycoprotein (LRG) can be a biomarker for the disease activity, progression, and prognosis of interstitial pneumonia (IP) in patients with dermatomyositis (DM).
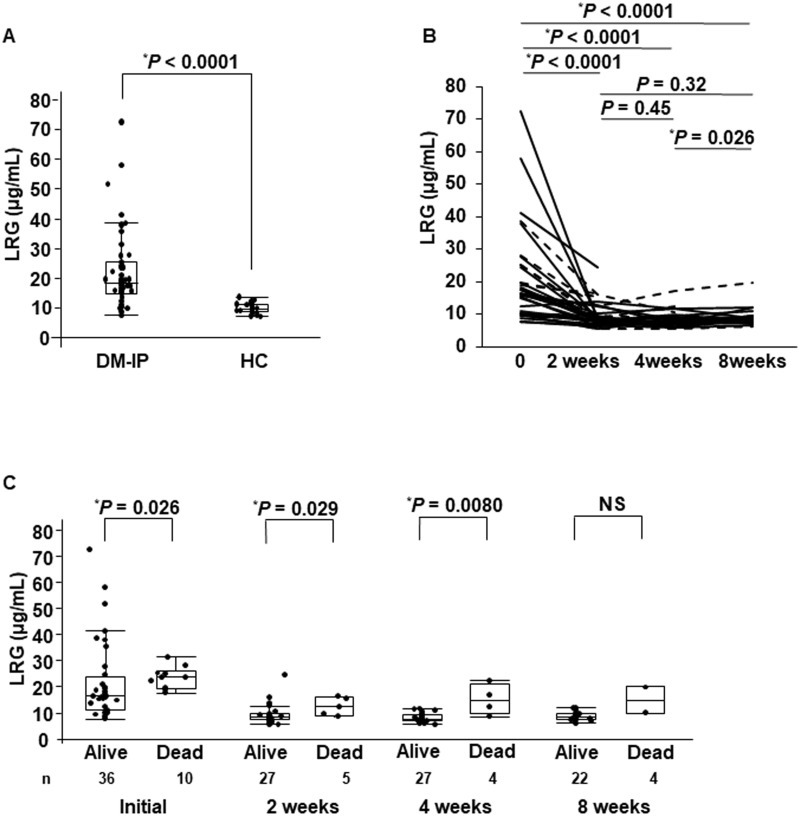
Methods: Correlations between the clinical findings and serum LRG levels were investigated in 46 patients with DM-IP (33 with acute/subacute IP [A/SIP] and 13 patients with chronic IP [CIP], including 10 fatal cases of IP).
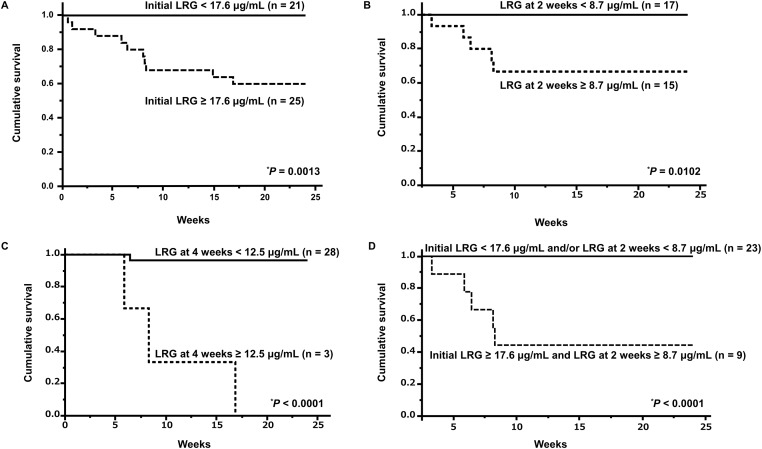
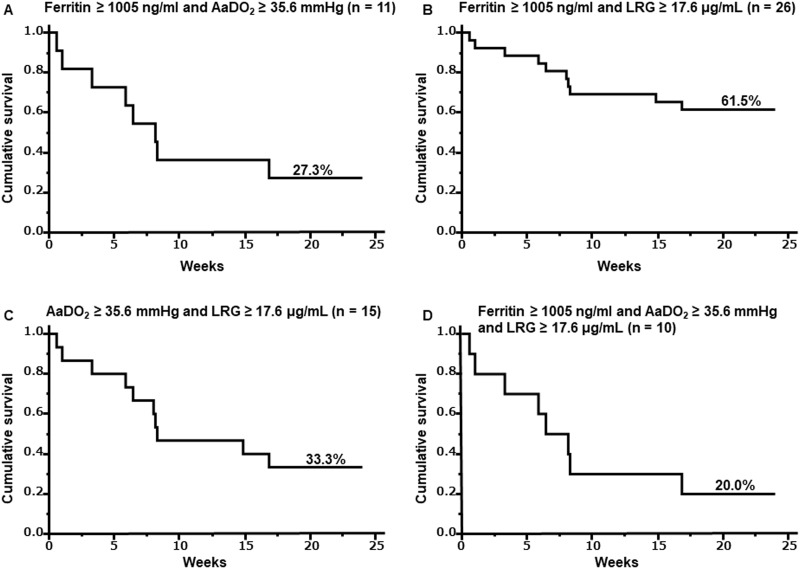
Results: The median serum LRG level of 18.4 (14.6-25.2) μg/mL in DM-IP patients was higher than that in healthy control subjects. The median levels of serum LRG at baseline and at 2 and 4 weeks after the initiation of treatment in the patients who died were significantly higher than those in the surviving patients (P = 0.026, 0.029, and 0.008, respectively). The median level of serum LRG in the DM-A/SIP patients was significantly higher than that in the DM-CIP patients (P = 0.0004), and that in the anti-MDA5-Ab-positive group was slightly higher than that in the anti-ARS-Ab-positive group. The serum LRG levels correlated significantly with the serum levels of LDH, C-reactive protein, ferritin, AaDO2, %DLco, and total ground-glass opacity score. The survival rate after 24 weeks in patients with an initial LRG level ≥ 17.6 μg/mL (survival rate: 40%) was significantly lower than that in patients with an initial LRG level < 17.6 μg/mL (100%) (P = 0.0009).
Conclusion: The serum LRG level may be a promising marker of disease activity, progression, and prognosis in patients with DM-IP.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Benbassat J, Gefel D, Larholt K, Sukenik S, Morgenstern V, Zlotnick A. Prognostic factors in polymyositis/dermatomyositis. A computer–assisted analysis of ninety-two cases. Arthritis Rheum. 1985; 28: 49–55. - PubMed
-
- Maugars YM, Berthelot JM, Abbas AA, Mussini JM, Nguyen JM, Prost AM. Long-term prognosis of 69 patients with dermatomyositis or polymyositis. Clin Exp Rheumatol. 1996; 14: 263–274. - PubMed
-
- Koreeda Y, Higashimoto I, Yamamoto M, Takahashi M, Kaji K, Fujimoto M, et al. Clinical and pathological findings of interstitial lung disease patients with anti-aminoacyl-tRNA synthetase autoantibodies. Intern Med. 2010; 49: 361–369. - PubMed
-
- Isoda K, Kotani T, Takeuchi T, Kiboshi T, Hata K, Ishida T, et al. Comparison of long-term prognosis and relapse of dermatomyositis complicated with interstitial pneumonia according to autoantibodies: anti-aminoacyl tRNA synthetase antibodies versus anti-melanoma differentiation-associated gene 5 antibody. Rheumatol Int. 2017; 37: 1335–1340. - PubMed
-
- Gono T, Kawaguchi Y, Satoh T, Kuwana M, Katsumata Y, Takagi K, et al. Clinical manifestation and prognostic factor in anti-melanoma differentiation-associated gene 5 antibody-associated interstitial lung disease as a complication of dermatomyositis. Rheumatology (Oxford). 2010; 49: 1713–1719. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
