

Hypertrophic scars and keloids: Overview of the evidence and practical guide for differentiating between these abnormal scars
- PMID: 32479693
- PMCID: PMC7818137
- DOI: 10.1111/exd.14121
Hypertrophic scars and keloids: Overview of the evidence and practical guide for differentiating between these abnormal scars
Abstract
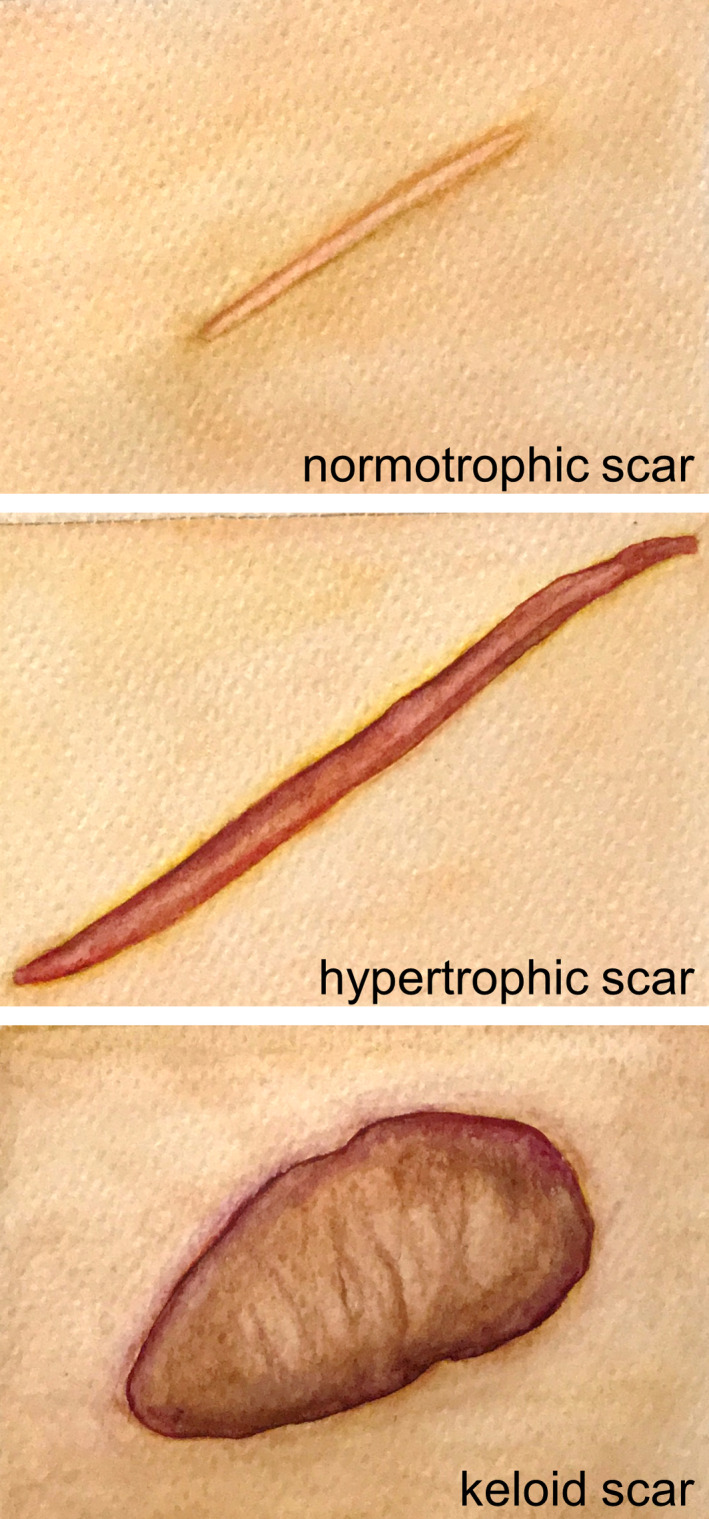
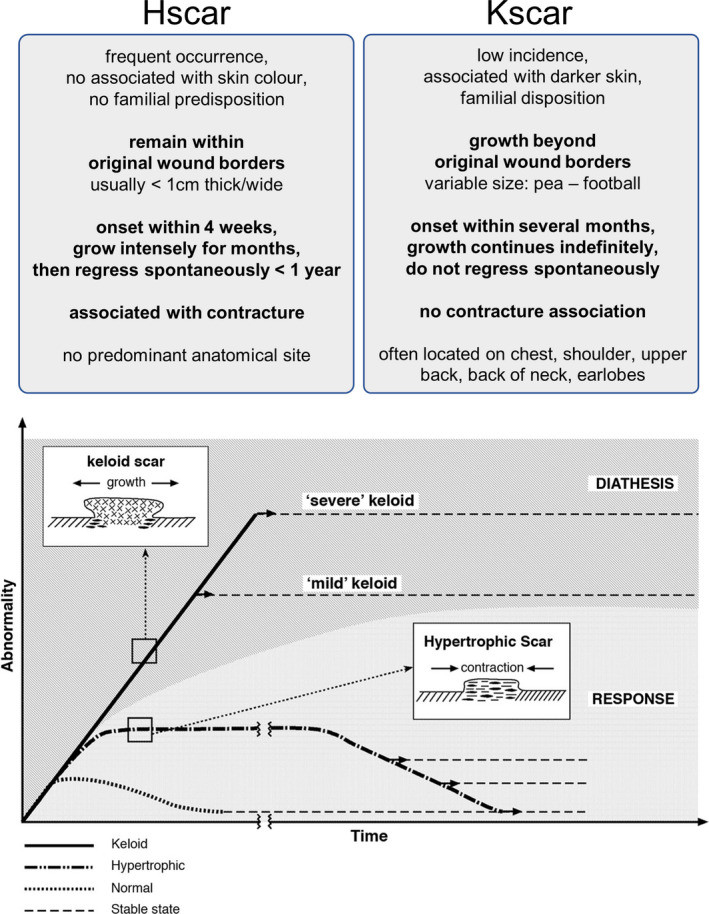
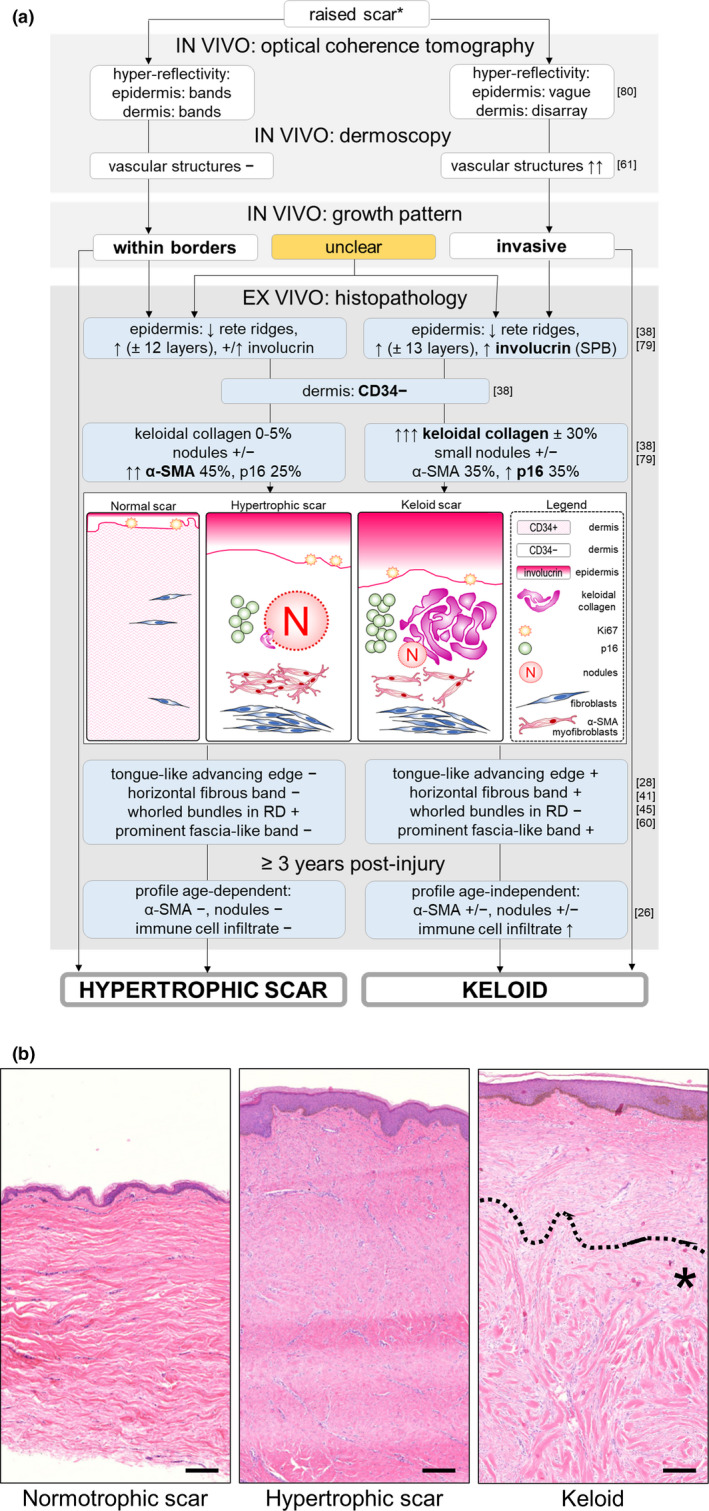
Although hypertrophic scars and keloids both generate excessive scar tissue, keloids are characterized by their extensive growth beyond the borders of the original wound, which is not observed in hypertrophic scars. Whether or not hypertrophic scars and keloids are two sides of the same coin or in fact distinct entities remains a topic of much debate. However, proper comparison between the two ideally occurs within the same study, but this is the exception rather than the rule. For this reason, the goal of this review was to summarize and evaluate all publications in which both hypertrophic scars and keloids were studied and compared to one another within the same study. The presence of horizontal growth is the mainstay of the keloid diagnosis and remains the strongest argument in support of keloids and hypertrophic scars being distinct entities, and the histopathological distinction is less straightforward. Keloidal collagen remains the strongest keloid parameter, but dermal nodules and α-SMA immunoreactivity are not limited to hypertrophic scars alone. Ultimately, the current hypertrophic scars-keloid differences are mostly quantitative in nature rather than qualitative, and many similar abnormalities exist in both lesions. Nonetheless, the presence of similarities does not equate the absence of fundamental differences, some of which may not yet have been uncovered given how much we still have to learn about the processes involved in normal wound healing. It therefore seems pertinent to continue treating hypertrophic scars and keloids as separate entities, until such a time as new findings more decisively convinces us otherwise.
Keywords: diagnosis; histopathology; hypertrophic; keloid; scar.
© 2020 The Authors. Experimental Dermatology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflicts of interests to declare.
Figures
References
-
- Wolfram D., Tzankov A., Pülzl P., Piza‐Katzer H., Dermatol. Surg. 2009, 35, 171. - PubMed
-
- Burd A., Huang L., Plast. Reconstr. Surg. 2005, 116, 150e. - PubMed
-
- Kumar V., Abbas A. K., Fausto N., In Robbins and Cotran, Pathologic Basis of Disease, 7th Edition (Eds: Kumar V., Abbas A. K., Fausto N.), Elsevier Saunders, Philadelphia, PA: 2004, Ch. 87‐118.
-
- Sorg H., Tilkorn D. J., Hager S., Hauser J., Mirastschijski U., Eur. Surg. Res. 2017, 58, 81. - PubMed
-
- Ghazawi F. M., Zargham R., Gilardino M. S., Sasseville D., Jafarian F., Adv. Skin. Wound Care 2018, 31, 582. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
