

Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: an international cohort study
- PMID: 32479829
- PMCID: PMC7259900
- DOI: 10.1016/S0140-6736(20)31182-X
Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: an international cohort study
Erratum in
-
Department of Error.Lancet. 2020 Jul 25;396(10246):238. doi: 10.1016/S0140-6736(20)31350-7. Epub 2020 Jun 9. Lancet. 2020. PMID: 32531186 Free PMC article. No abstract available.
Abstract
Background: The impact of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on postoperative recovery needs to be understood to inform clinical decision making during and after the COVID-19 pandemic. This study reports 30-day mortality and pulmonary complication rates in patients with perioperative SARS-CoV-2 infection.
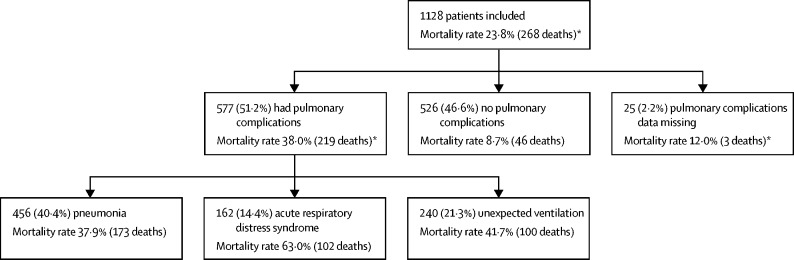
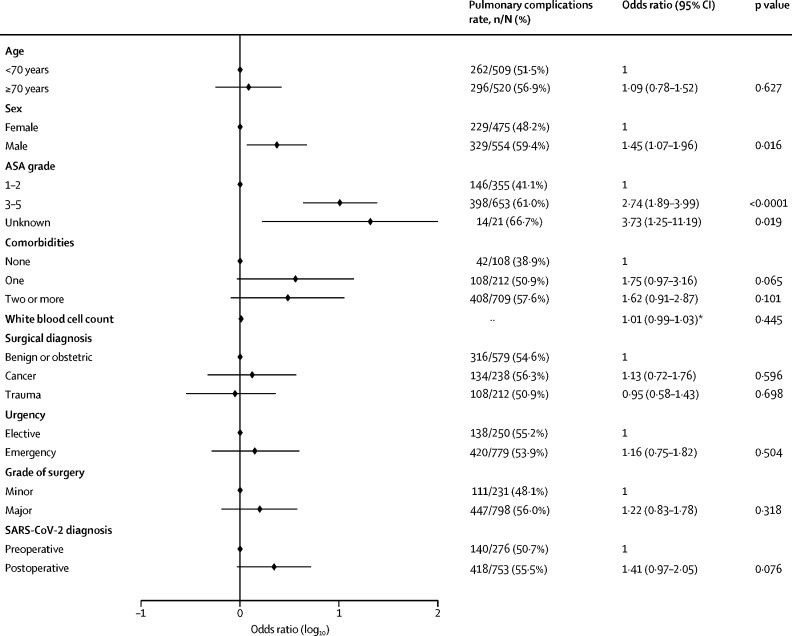
Methods: This international, multicentre, cohort study at 235 hospitals in 24 countries included all patients undergoing surgery who had SARS-CoV-2 infection confirmed within 7 days before or 30 days after surgery. The primary outcome measure was 30-day postoperative mortality and was assessed in all enrolled patients. The main secondary outcome measure was pulmonary complications, defined as pneumonia, acute respiratory distress syndrome, or unexpected postoperative ventilation.
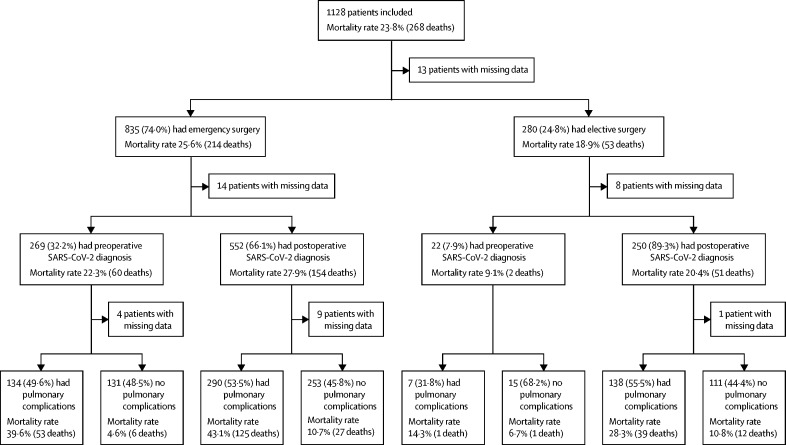
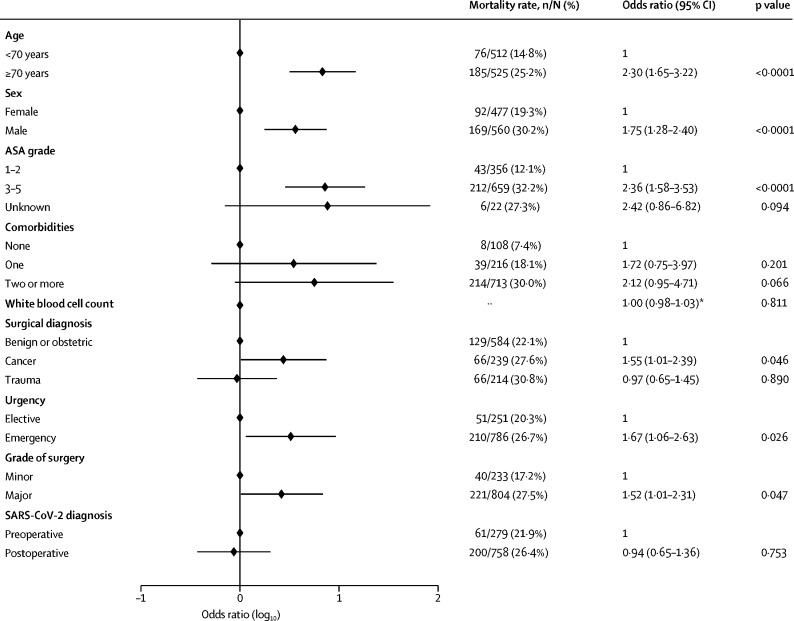
Findings: This analysis includes 1128 patients who had surgery between Jan 1 and March 31, 2020, of whom 835 (74·0%) had emergency surgery and 280 (24·8%) had elective surgery. SARS-CoV-2 infection was confirmed preoperatively in 294 (26·1%) patients. 30-day mortality was 23·8% (268 of 1128). Pulmonary complications occurred in 577 (51·2%) of 1128 patients; 30-day mortality in these patients was 38·0% (219 of 577), accounting for 81·7% (219 of 268) of all deaths. In adjusted analyses, 30-day mortality was associated with male sex (odds ratio 1·75 [95% CI 1·28-2·40], p<0·0001), age 70 years or older versus younger than 70 years (2·30 [1·65-3·22], p<0·0001), American Society of Anesthesiologists grades 3-5 versus grades 1-2 (2·35 [1·57-3·53], p<0·0001), malignant versus benign or obstetric diagnosis (1·55 [1·01-2·39], p=0·046), emergency versus elective surgery (1·67 [1·06-2·63], p=0·026), and major versus minor surgery (1·52 [1·01-2·31], p=0·047).
Interpretation: Postoperative pulmonary complications occur in half of patients with perioperative SARS-CoV-2 infection and are associated with high mortality. Thresholds for surgery during the COVID-19 pandemic should be higher than during normal practice, particularly in men aged 70 years and older. Consideration should be given for postponing non-urgent procedures and promoting non-operative treatment to delay or avoid the need for surgery.
Funding: National Institute for Health Research (NIHR), Association of Coloproctology of Great Britain and Ireland, Bowel and Cancer Research, Bowel Disease Research Foundation, Association of Upper Gastrointestinal Surgeons, British Association of Surgical Oncology, British Gynaecological Cancer Society, European Society of Coloproctology, NIHR Academy, Sarcoma UK, Vascular Society for Great Britain and Ireland, and Yorkshire Cancer Research.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Mitigating the risks of surgery during the COVID-19 pandemic.Lancet. 2020 Jul 4;396(10243):2-3. doi: 10.1016/S0140-6736(20)31256-3. Epub 2020 May 29. Lancet. 2020. PMID: 32479826 Free PMC article. No abstract available.
-
Surgery during the COVID-19 pandemic.Lancet. 2020 Nov 7;396(10261):e73. doi: 10.1016/S0140-6736(20)32281-9. Lancet. 2020. PMID: 33160573 Free PMC article. No abstract available.
-
Surgery during the COVID-19 pandemic.Lancet. 2020 Nov 7;396(10261):e74. doi: 10.1016/S0140-6736(20)32279-0. Lancet. 2020. PMID: 33160574 Free PMC article. No abstract available.
-
Surgery during the COVID-19 pandemic.Lancet. 2020 Nov 7;396(10261):e75. doi: 10.1016/S0140-6736(20)32280-7. Lancet. 2020. PMID: 33160575 Free PMC article. No abstract available.
-
Surgery during the COVID-19 pandemic.Lancet. 2020 Nov 7;396(10261):e76. doi: 10.1016/S0140-6736(20)32278-9. Lancet. 2020. PMID: 33160576 Free PMC article. No abstract available.
-
Surgery during the COVID-19 pandemic.Lancet. 2020 Nov 7;396(10261):e77. doi: 10.1016/S0140-6736(20)32277-7. Lancet. 2020. PMID: 33160577 Free PMC article. No abstract available.
-
Surgery during the COVID-19 pandemic.Lancet. 2020 Nov 7;396(10261):e78. doi: 10.1016/S0140-6736(20)32276-5. Lancet. 2020. PMID: 33160578 Free PMC article. No abstract available.
-
Mortality in patients undergoing surgery with perioperative SARS-CoV-2 infection: an Italian COVID-19 Hub point of view.Eur Rev Med Pharmacol Sci. 2020 Nov;24(22):11471-11473. doi: 10.26355/eurrev_202011_23786. Eur Rev Med Pharmacol Sci. 2020. PMID: 33275211 No abstract available.
References
-
- WHO WHO announces COVID-19 outbreak a pandemic. March 12, 2020. http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-...
-
- Kirmeier E, Eriksson LI, Lewald H. Post-anaesthesia pulmonary complications after use of muscle relaxants (POPULAR): a multicentre, prospective observational study. Lancet Respir Med. 2019;7:129–140. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
