

Percutaneous pedicle screw fixation combined with transforaminal endoscopic spinal canal decompression for the treatment of thoracolumbar burst fracture with severe neurologic deficit: A case report
- PMID: 32481306
- PMCID: PMC7249900
- DOI: 10.1097/MD.0000000000020276
Percutaneous pedicle screw fixation combined with transforaminal endoscopic spinal canal decompression for the treatment of thoracolumbar burst fracture with severe neurologic deficit: A case report
Abstract
Rationale: The most common fractures of the spine are associated with the thoracolumbar junction (T10-L2). And burst fractures make up 15% of all traumatic thoracolumbar fractures, which are often accompanied by neurological deficits and require open surgeries. Common surgeries include either anterior, posterior or a combination of these approaches. Here, we report the first attempt to treat thoracolumbar burst fracture (TLBF) with severe neurologic deficits by percutaneous pedicle screw fixation (PPSF) and transforaminal endoscopic spinal canal decompression (TESCD).
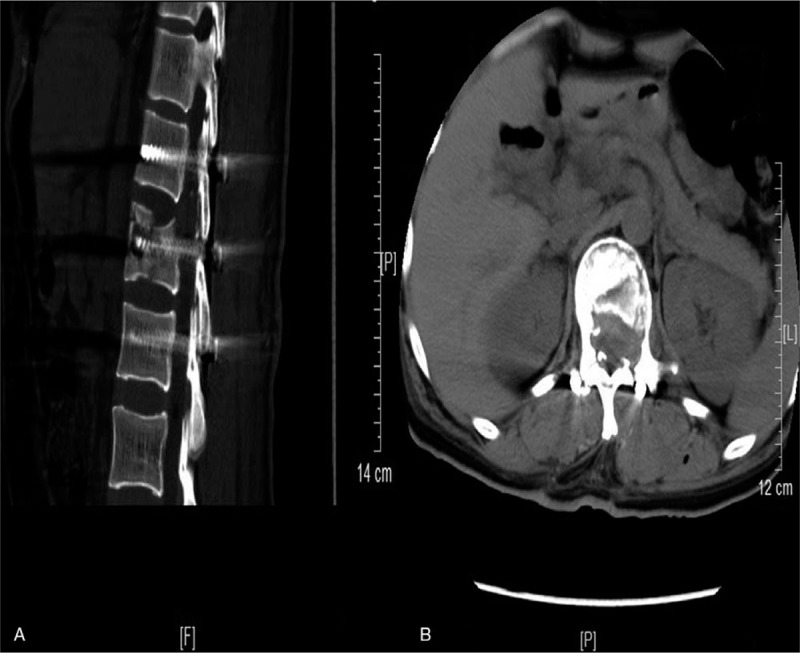
Patient concerns: A 46-year-old Chinese woman suffered from severe lower back pain with grade 0 muscle strength of lower limbs, without any sensory function below the injury level, with an inability to urinate or defecate after a motor vehicle accident. Imaging studies confirmed that she had Magerl type A 3.2 L1 burst fracture.
Diagnoses: Burst fracture at L1.
Interventions: The patient underwent PPSF at the level of T12 to L2, but her neurological function did not fully recover after the operation. One week after the injury, we performed TESCD on her.
Outcomes: There was an immediate improvement in her neurological function in just 1 day after 2-stage operation. During the 6-month follow-up period, her neurological functions gradually recovered, and she was able to defecate and urinate. At the last follow-up visit, her spinal cord function was assessed to be at Frankel grade D.
Lessons: PPSF plus TESCD can achieve complete spinal cord decompression, promote neurological recovery, and is therefore an effective method for the treating lumbar burst fractures with severe neurologic deficits.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



References
-
- Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983;8:817–31. - PubMed
-
- Dai LY, Yao WF, Cui YM, et al. Thoracolumbar fractures in patients with multiple injuries: diagnosis and treatment-a review of 147 cases. J Trauma 2004;56:348–55. - PubMed
-
- Phan K, Rao PJ, Mobbs RJ. Percutaneous versus open pedicle screw fixation for treatment of thoracolumbar fractures: Systematic review and meta-analysis of comparative studies. Clin Neurol Neurosurg 2015;135:85–92. - PubMed
-
- McLain RF. Functional outcomes after surgery for spinal fractures: return to work and activity. Spine 2004;29:470–7. discussion Z6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
