

Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry
- PMID: 32482845
- PMCID: PMC7668545
- DOI: 10.1212/WNL.0000000000009937
Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry
Abstract
Objective: The coronavirus disease 2019 (COVID-19) has spread worldwide since December 2019. Neurologic symptoms have been reported as part of the clinical spectrum of the disease. We aimed to determine whether neurologic manifestations are common in hospitalized patients with COVID-19 and to describe their main characteristics.
Methods: We systematically reviewed all patients diagnosed with COVID-19 admitted to the hospital in a Spanish population during March 2020. Demographic characteristics, systemic and neurologic clinical manifestations, and complementary tests were analyzed.
Results: Of 841 patients hospitalized with COVID-19 (mean age 66.4 years, 56.2% men), 57.4% developed some form of neurologic symptom. Nonspecific symptoms such as myalgias (17.2%), headache (14.1%), and dizziness (6.1%) were present mostly in the early stages of infection. Anosmia (4.9%) and dysgeusia (6.2%) tended to occur early (60% as the first clinical manifestation) and were more frequent in less severe cases. Disorders of consciousness occurred commonly (19.6%), mostly in older patients and in severe and advanced COVID-19 stages. Myopathy (3.1%), dysautonomia (2.5%), cerebrovascular diseases (1.7%), seizures (0.7%), movement disorders (0.7%), encephalitis (n = 1), Guillain-Barré syndrome (n = 1), and optic neuritis (n = 1) were also reported, but less frequent. Neurologic complications were the main cause of death in 4.1% of all deceased study participants.
Conclusions: Neurologic manifestations are common in hospitalized patients with COVID-19. In our series, more than half of patients presented some form of neurologic symptom. Clinicians need to maintain close neurologic surveillance for prompt recognition of these complications. The mechanisms and consequences of severe acute respiratory syndrome coronavirus type 2 neurologic involvement require further studies.
© 2020 American Academy of Neurology.
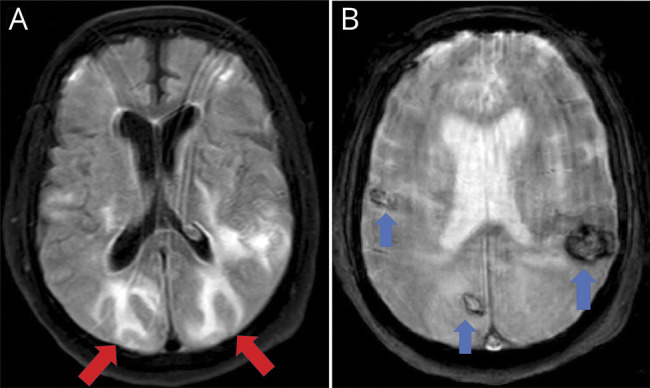
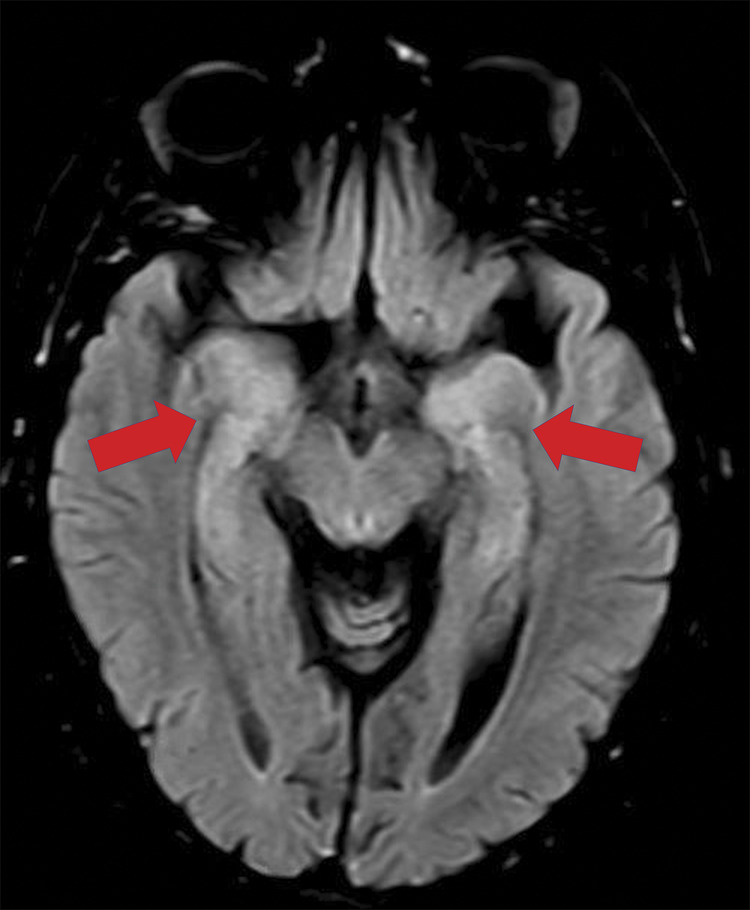
Figures
Similar articles
-
Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China.JAMA Neurol. 2020 Jun 1;77(6):683-690. doi: 10.1001/jamaneurol.2020.1127. JAMA Neurol. 2020. PMID: 32275288 Free PMC article.
-
Environmental Issues and Neurological Manifestations Associated with COVID-19 Pandemic: New Aspects of the Disease?Int J Environ Res Public Health. 2020 Nov 1;17(21):8049. doi: 10.3390/ijerph17218049. Int J Environ Res Public Health. 2020. PMID: 33139595 Free PMC article. Review.
-
Neurological manifestations and complications of COVID-19: A literature review.J Clin Neurosci. 2020 Jul;77:8-12. doi: 10.1016/j.jocn.2020.05.017. Epub 2020 May 6. J Clin Neurosci. 2020. PMID: 32409215 Free PMC article. Review.
-
Frequent neurologic manifestations and encephalopathy-associated morbidity in Covid-19 patients.Ann Clin Transl Neurol. 2020 Nov;7(11):2221-2230. doi: 10.1002/acn3.51210. Epub 2020 Oct 5. Ann Clin Transl Neurol. 2020. PMID: 33016619 Free PMC article.
-
Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review.JAMA Neurol. 2020 Aug 1;77(8):1018-1027. doi: 10.1001/jamaneurol.2020.2065. JAMA Neurol. 2020. PMID: 32469387 Free PMC article. Review.
Cited by
-
COVID-19 and its implications on the clinico-radiological course of multiple sclerosis: A case-control study.Med Clin (Barc). 2023 Mar 10;160(5):187-192. doi: 10.1016/j.medcli.2022.06.020. Epub 2022 Aug 10. Med Clin (Barc). 2023. PMID: 36089420 Free PMC article.
-
Parkinsonism as a Third Wave of the COVID-19 Pandemic?J Parkinsons Dis. 2020;10(4):1343-1353. doi: 10.3233/JPD-202211. J Parkinsons Dis. 2020. PMID: 32986683 Free PMC article.
-
Inpatient outcomes of inflammatory bowel disease in hospitalized patients with COVID-19: analysis of a nationally representative sample.Proc (Bayl Univ Med Cent). 2024 Feb 8;37(2):239-247. doi: 10.1080/08998280.2024.2303402. eCollection 2024. Proc (Bayl Univ Med Cent). 2024. PMID: 38343460 Free PMC article.
-
Brain stem encephalitis is a rare complication of COVID-19.J Neuroimmunol. 2023 Jan 15;374:578007. doi: 10.1016/j.jneuroim.2022.578007. Epub 2022 Nov 28. J Neuroimmunol. 2023. PMID: 36481703 Free PMC article.
-
High-dose steroid-responsive COVID-19-related encephalopathy with a sudden onset of dysarthria mimicking stroke: a case report.J Cent Nerv Syst Dis. 2022 Dec 22;14:11795735221147218. doi: 10.1177/11795735221147218. eCollection 2022. J Cent Nerv Syst Dis. 2022. PMID: 36579076 Free PMC article.
References
-
- World Health Organization. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19. Geneva: World Health Organization; 2020.
-
- Johns Hopkins University and Medicine. COVID-19 Map. Johns Hopkins Coronavirus Resource Centre. Available at: coronavirus.jhu.edu/map.html. Accessed April 30, 2020.
-
- Baig AM, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem Neurosci 2020;11:995–998. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical