

Immunohistochemical PSMA expression patterns of primary prostate cancer tissue are associated with the detection rate of biochemical recurrence with 68Ga-PSMA-11-PET
- PMID: 32483440
- PMCID: PMC7255040
- DOI: 10.7150/thno.44584
Immunohistochemical PSMA expression patterns of primary prostate cancer tissue are associated with the detection rate of biochemical recurrence with 68Ga-PSMA-11-PET
Abstract
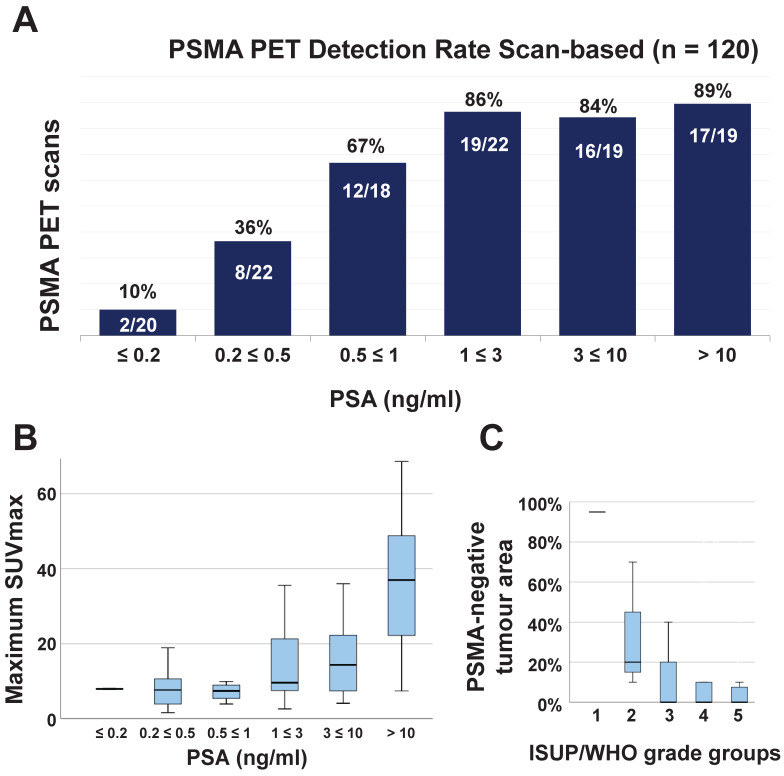
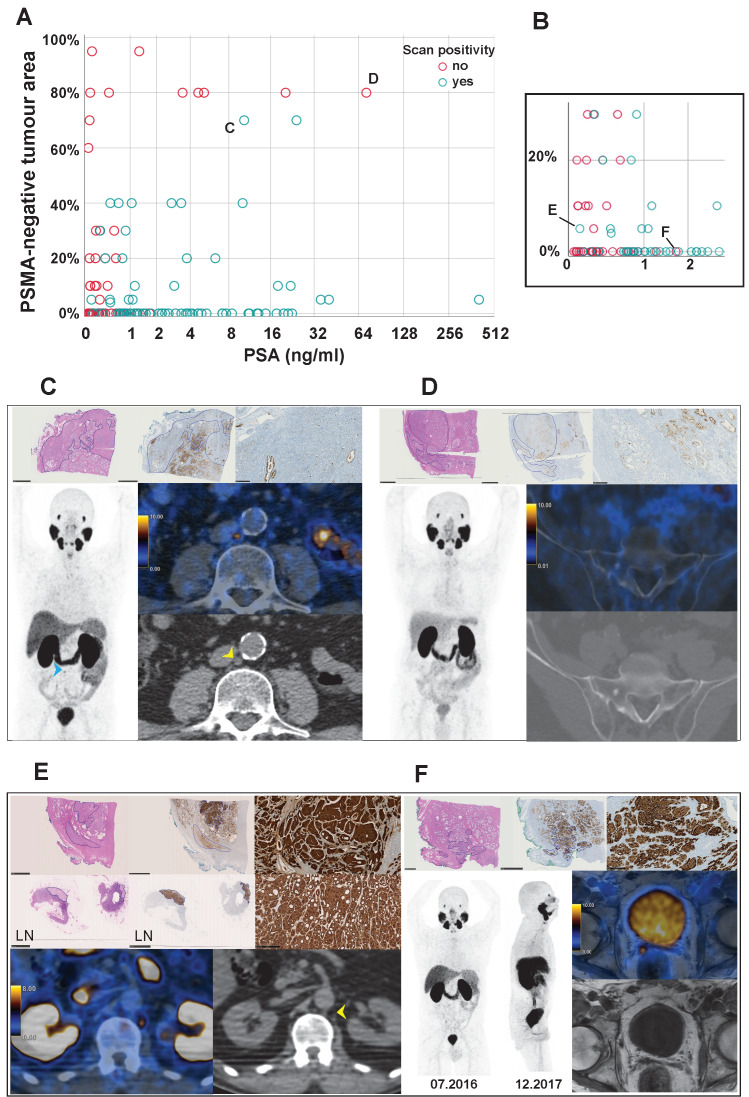
Prostate-specific membrane antigen (PSMA) targeted PET has a high detection rate for biochemical recurrence (BCR) of prostate cancer (PCa). Nevertheless, even at high prostate-specific antigen (PSA) levels (> 3 ng/ml), a relevant number of PSMA-PET scans are negative, mainly due to PSMA-negative PCa. Our objective was to investigate whether PSMA-expression patterns of the primary tumour on immunohistochemistry (IHC) are associated with PSMA-PET detection rate of recurrent PCa. Methods: Retrospective institutional review board approved single-centre analysis of patients who had undergone 68Ga-PSMA-11-PET for BCR after radical prostatectomy (RPE) between 04/2016 and 07/2019, with tumour specimens available for PSMA-IHC. Clinical information (age, PSA-level, ongoing androgen deprivation therapy (ADT), Gleason score) and PSMA-IHC of the primary tumour were collected and their relationship to results from PSMA-PET (positive/negative) was investigated using a multiple logistic regression analysis. Results: 120 PSMA-PET scans in 74 patients were available for this analysis. Overall detection rate was 62% (74/120 scans), with a mean PSA value at scan time of 0.99 ng/ml (IQR 0.32-4.27). Of the clinical factors, only PSA-level and ADT were associated with PSMA-PET positivity. The percentage of PSMA-negative tumour area on IHC (PSMA%neg) had a significant association to PSMA-PET negativity (OR = 2.88, p < 0.001), while membranous PSMA-expression showed no association (p = 0.73). The positive predictive value of PSMA%neg ≥ 50% for a negative PSMA-PET was 85% (13/11) and for a PSMA%neg of 80% or more, 100% (9/9). Conclusions: PSMA-negative tumour area on IHC exhibited the strongest association with negative PSMA-PET scans, beside PSA-level and ADT. Even at very high PSA levels, PSMA-PET scans were negative in most of the patients with PSMA%neg ≥ 50%.
Keywords: PSMA PET; PSMA staining; PSMA-negative prostate cancer; immunohistochemistry; restaging.
© The author(s).
Conflict of interest statement
Competing Interests: IAB has received research grants and speaker honorarium from GE Healthcare, research grants from Swiss Life and speaker honorarium from Bayer Health Care and Astellas Pharma AG. MM received speaker fees from GE Healthcare. TH holds an advisory function for MSD and Bayer. Authors DAF, JHR, UJM, BK, JM, LH, DE, and NJR declare no conflict of interest. The Department of Nuclear Medicine holds an institutional Research Contract with GE Healthcare. The authors thank the Sick legat and the Iten-Kohaut foundation for their financial support.
Figures



References
-
- Wright GL Jr, Haley C, Beckett ML, Schellhammer PF. Expression of prostate-specific membrane antigen in normal, benign, and malignant prostate tissues. Urol Oncol. 1995;1:18–28. - PubMed
-
- Bostwick DG, Pacelli A, Blute M, Roche P, Murphy GP. Prostate specific membrane antigen expression in prostatic intraepithelial neoplasia and adenocarcinoma - A study of 184 cases. Cancer. 1998;82:2256–61. - PubMed
-
- Silver DA, Pellicer I, Fair WR, Heston WD, Cordon-Cardo C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin Cancer Res. 1997;3:81–5. - PubMed
-
- Sweat SD, Pacelli A, Murphy GP, Bostwick DG. Prostate-specific membrane antigen expression is greatest in prostate adenocarcinoma and lymph node metastases. Urology. 1998;52:637–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
