

Effect of C-Reactive Protein-Guided Antibiotic Treatment Duration, 7-Day Treatment, or 14-Day Treatment on 30-Day Clinical Failure Rate in Patients With Uncomplicated Gram-Negative Bacteremia: A Randomized Clinical Trial
- PMID: 32484534
- PMCID: PMC7267846
- DOI: 10.1001/jama.2020.6348
Effect of C-Reactive Protein-Guided Antibiotic Treatment Duration, 7-Day Treatment, or 14-Day Treatment on 30-Day Clinical Failure Rate in Patients With Uncomplicated Gram-Negative Bacteremia: A Randomized Clinical Trial
Abstract
Importance: Antibiotic overuse drives antibiotic resistance. Gram-negative bacteremia is a common infection that results in substantial antibiotic use.
Objective: To compare the clinical effectiveness of C-reactive protein (CRP)-guided, 7-day, and 14-day antibiotic durations 30, 60, and 90 days after treatment initiation.
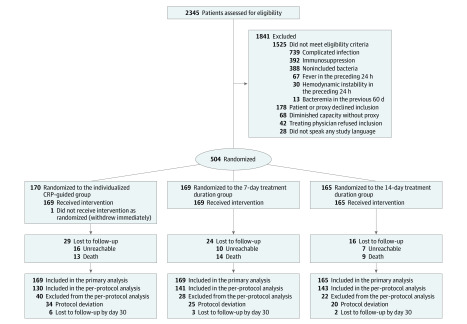
Design, setting, and participants: Multicenter, noninferiority, point-of-care randomized clinical trial including adults hospitalized with gram-negative bacteremia conducted in 3 Swiss tertiary care hospitals between April 2017 and May 2019, with follow-up until August 2019. Patients and physicians were blinded between randomization and antibiotic discontinuation. Adults (aged ≥18 years) were eligible for randomization on day 5 (±1 d) of microbiologically efficacious therapy for fermenting, gram-negative bacteria in blood culture(s) if they were afebrile for 24 hours without evidence for complicated infection (eg, abscess) or severe immunosuppression.
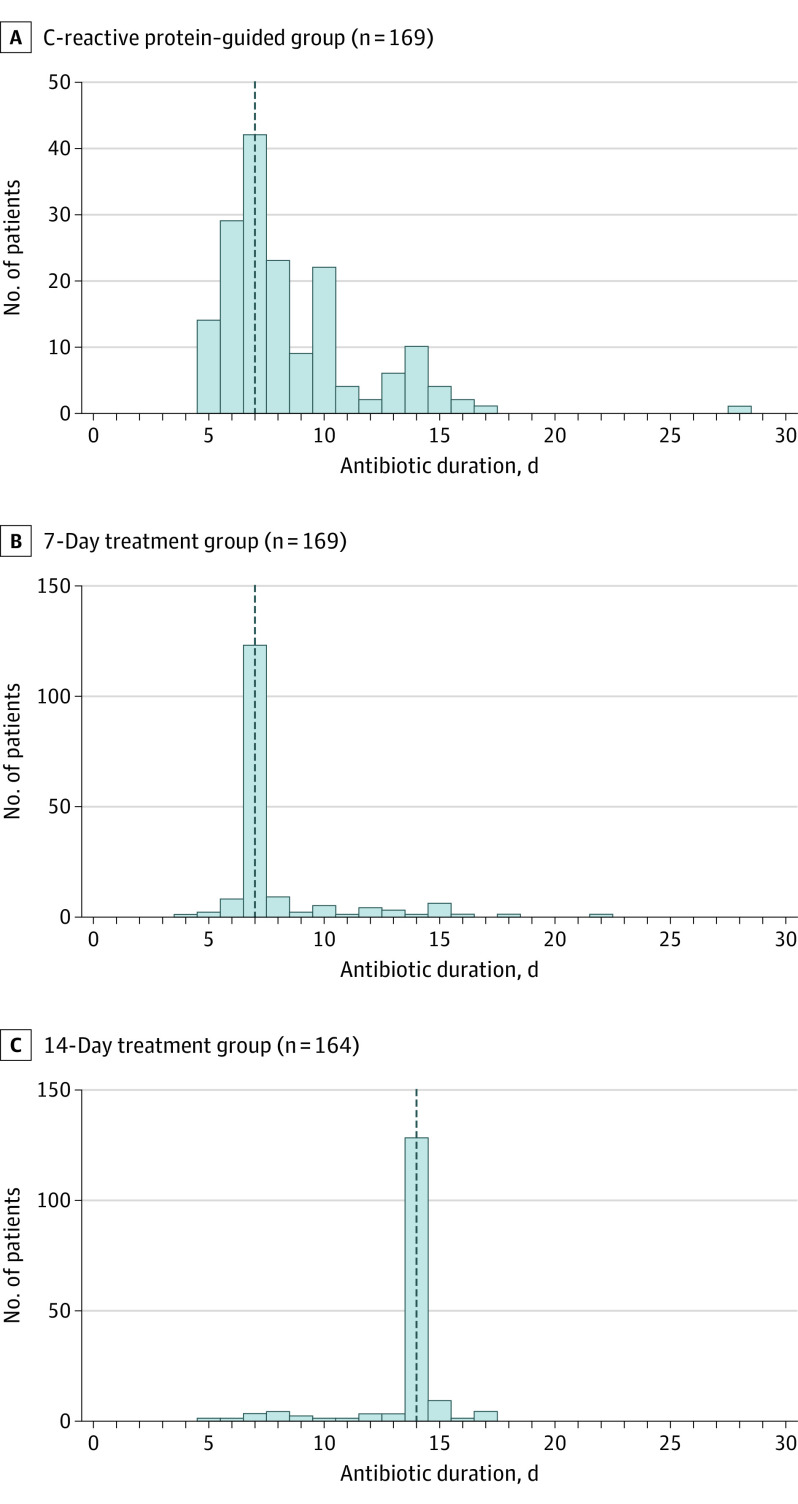
Intervention: Randomization in a 1:1:1 ratio to an individualized CRP-guided antibiotic treatment duration (discontinuation once CRP declined by 75% from peak; n = 170), fixed 7-day treatment duration (n = 169), or fixed 14-day treatment duration (n = 165).
Main outcomes and measures: The primary outcome was the clinical failure rate at day 30, defined as the presence of at least 1 of the following, with a non-inferiority margin of 10%: recurrent bacteremia, local suppurative complication, distant complication (growth of the same organism causing the initial bacteremia), restarting gram-negative-directed antibiotic therapy due to clinical worsening suspected to be due to the initial organism, or death due to any cause. Secondary outcomes included the clinical failure rate on day 90 of follow-up.
Results: Among 504 patients randomized (median [interquartile range] age, 79 [68-86] years; 306 of 503 [61%] were women), 493 (98%) completed 30-day follow-up and 448 (89%) completed 90-day follow-up. Median antibiotic duration in the CRP group was 7 (interquartile range, 6-10; range, 5-28) days; 34 of the 164 patients (21%) who completed the 30-day follow-up had protocol violations related to treatment assignment. The primary outcome occurred in 4 of 164 (2.4%) patients in the CRP group, 11 of 166 (6.6%) in the 7-day group, and 9 of 163 (5.5%) in the 14-day group (difference in CRP vs 14-day group, -3.1% [1-sided 97.5% CI, -∞ to 1.1]; P < .001; difference in 7-day vs 14-day group, 1.1% [1-sided 97.5% CI, -∞ to 6.3]; P < .001). By day 90, clinical failure occurred in 10 of 143 patients (7.0%) in the CRP group, 16 of 151 (10.6%) in the 7-day group, and 16 of 153 (10.5%) in the 14-day group.
Conclusions and relevance: Among adults with uncomplicated gram-negative bacteremia, 30-day rates of clinical failure for CRP-guided antibiotic treatment duration and fixed 7-day treatment were noninferior to fixed 14-day treatment. However, interpretation is limited by the large noninferiority margin compared with the low observed event rate, as well as low adherence and wide range of treatment durations in the CRP-guided group.
Trial registration: ClinicalTrials.gov Identifier: NCT03101072.
Conflict of interest statement
Figures
References
-
- Chotiprasitsakul D, Han JH, Cosgrove SE, et al. ; Antibacterial Resistance Leadership Group . Comparing the outcomes of adults with Enterobacteriaceae bacteremia receiving short-course versus prolonged-course antibiotic therapy in a multicenter, propensity score-matched cohort. Clin Infect Dis. 2018;66(2):172-177. doi: 10.1093/cid/cix767 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
