

Diagnostic performances and thresholds: The key to harmonization in serological SARS-CoV-2 assays?
- PMID: 32485157
- PMCID: PMC7261100
- DOI: 10.1016/j.cca.2020.05.050
Diagnostic performances and thresholds: The key to harmonization in serological SARS-CoV-2 assays?
Abstract
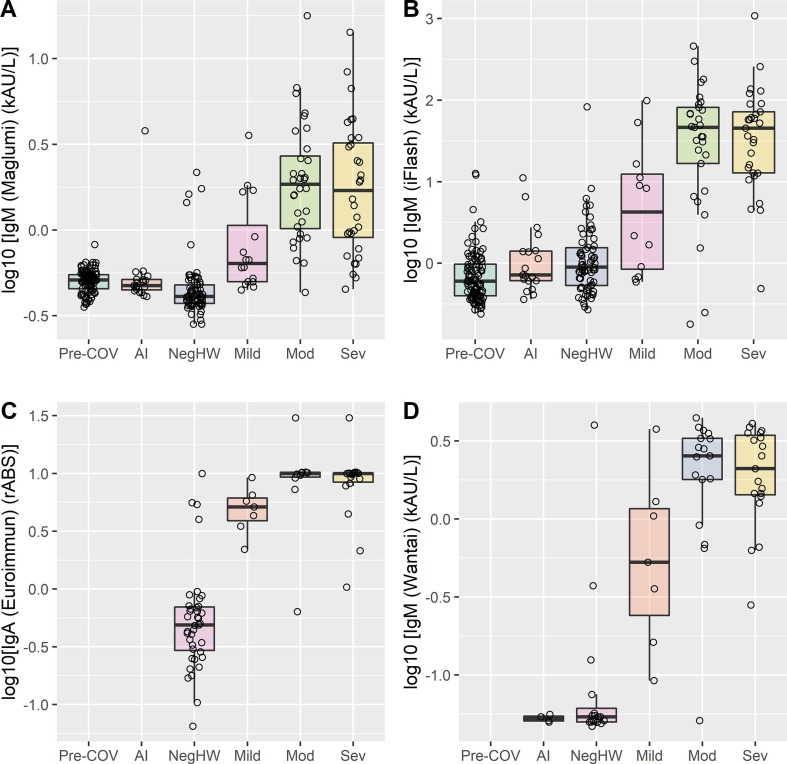
Background: The evaluation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) specific antibody (Ab) assay performances is of the utmost importance in establishing and monitoring virus spread in the community. In this study focusing on IgG antibodies, we compare reliability of three chemiluminescent (CLIA) and two enzyme linked immunosorbent (ELISA) assays.
Methods: Sera from a total of 271 subjects, including 64 reverse transcription-polymerase chain reaction (RT-PCR) confirmed SARS-CoV-2 patients were tested for specific Ab using Maglumi (Snibe), Liaison (Diasorin), iFlash (Yhlo), Euroimmun (Medizinische Labordiagnostika AG) and Wantai (Wantai Biological Pharmacy) assays. Diagnostic sensitivity and specificity, positive and negative likelihood ratios were evaluated using manufacturers' and optimized thresholds.
Results: Optimized thresholds (Maglumi 2 kAU/L, Liaison 6.2 kAU/L and iFlash 15.0 kAU/L) allowed us to achieve a negative likelihood ratio and an accuracy of: 0.06 and 93.5% for Maglumi; 0.03 and 93.1% for Liaison; 0.03 and 91% for iFlash. Diagnostic sensitivities and specificities were above 93.8% and 85.9%, respectively for all CLIA assays. Overall agreement was 90.3% (Cohen's kappa = 0.805 and SE = 0.041) for CLIA, and 98.4% (Cohen's kappa = 0.962 and SE = 0.126) for ELISA.
Conclusions: The results obtained indicate that, for CLIA assays, it might be possible to define thresholds that improve the negative likelihood ratio. Thus, a negative test result enables the identification of subjects at risk of being infected, who should then be closely monitored over time with a view to preventing further viral spread. Redefined thresholds, in addition, improved the overall inter-assay agreement, paving the way to a better harmonization of serologic tests.
Keywords: Antibodies; COVID-19; Clinical performances; SARS-CoV-2.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Sethuraman N, Jeremiah SS, Ryo A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020,(ahead of print) doi: 10.1001/jama.2020.8259. - PubMed
-
- Long QX, Liu BZ, Deng HJ, Wu GC, Deng K, Chen YK, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat Med 2020, (ahead of print) doi: 10.1038/s41591-020-0897-1. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
