

Temporal Trends in Prevalence and Prognostic Implications of Comorbidities Among Patients With Acute Decompensated Heart Failure: The ARIC Study Community Surveillance
- PMID: 32486833
- PMCID: PMC7654711
- DOI: 10.1161/CIRCULATIONAHA.120.047019
Temporal Trends in Prevalence and Prognostic Implications of Comorbidities Among Patients With Acute Decompensated Heart Failure: The ARIC Study Community Surveillance
Abstract
Background: Patients with heart failure (HF) have multiple coexisting comorbidities. The temporal trends in the burden of comorbidities and associated risk of mortality among patients with HF with preserved ejection fraction (HFpEF) and HF with reduced ejection fraction (HFrEF) are not well established.
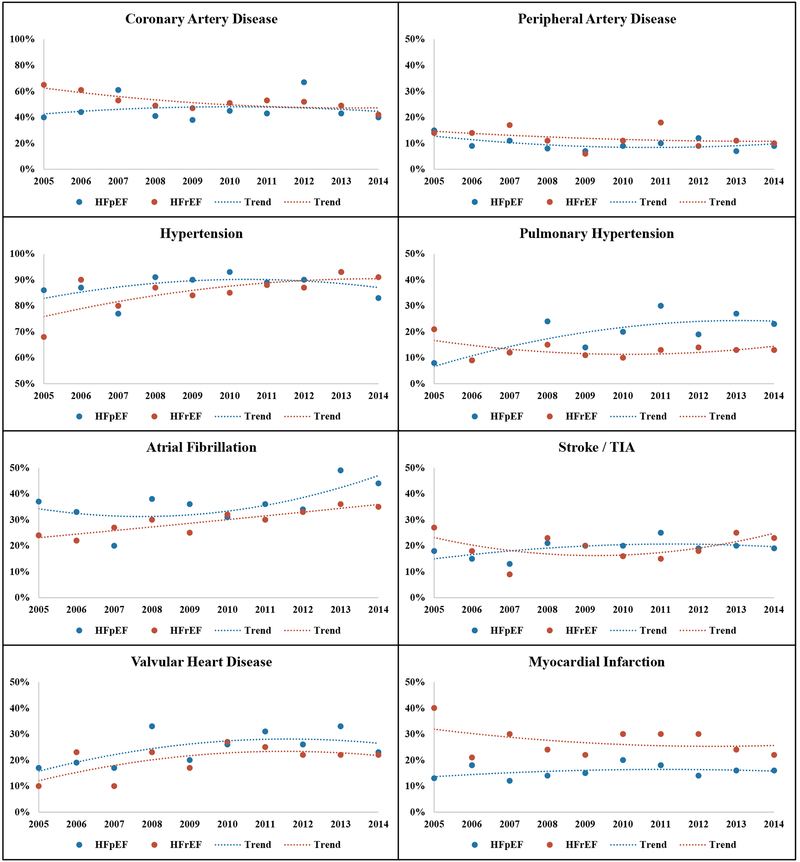
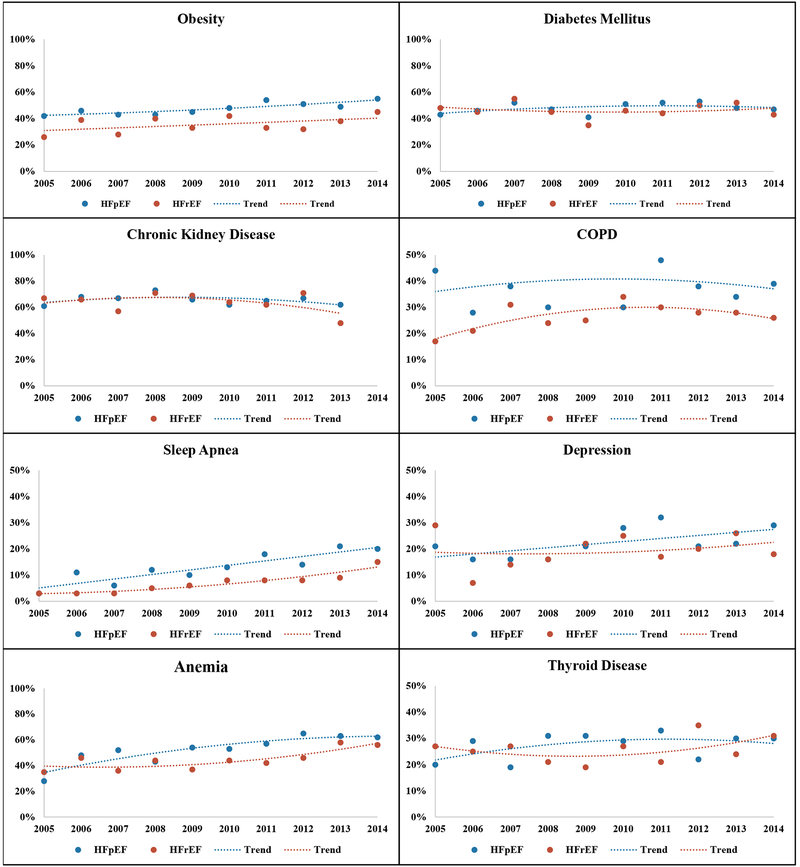
Methods: HF-related hospitalizations were sampled by stratified design from 4 US areas in 2005 to 2014 by the community surveillance component of the ARIC study (Atherosclerosis Risk in Communities). Acute decompensated HF was classified by standardized physician review and a previously validated algorithm. An ejection fraction <50% was considered HFrEF. A total of 15 comorbidities were abstracted from the medical record. Mortality outcomes were ascertained for up to 1-year postadmission by linking hospital records with death files.
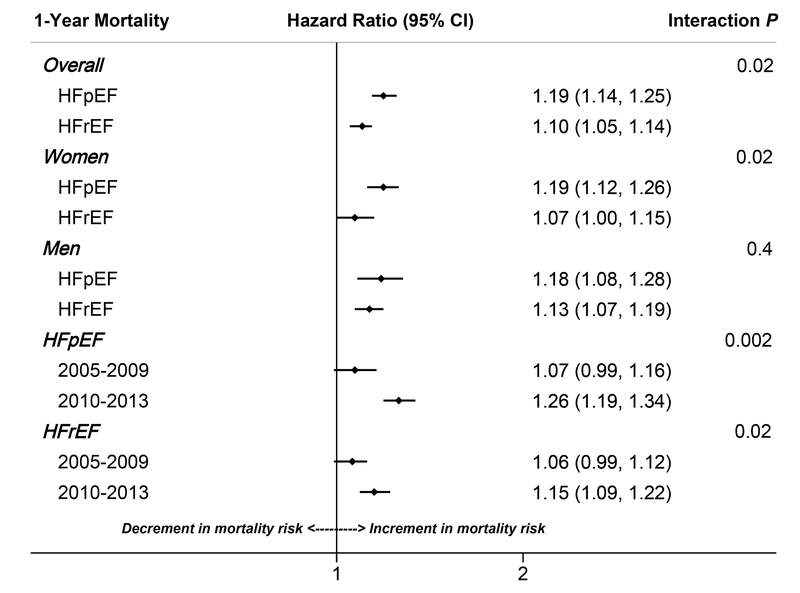
Results: A total of 5460 hospitalizations (24 937 weighted hospitalizations) classified as acute decompensated HF had available ejection fraction data (53% female, 68% white, 53% HFrEF, 47% HFpEF). The average number of comorbidities was higher for patients with HFpEF versus HFrEF, both for women (5.53 versus 4.94; P<0.0001) and men (5.20 versus 4.82; P<0.0001). There was a significant temporal increase in the overall burden of comorbidities, both for patients with HFpEF (women: 5.17 in 2005-2009 to 5.87 in 2010-2013; men: 4.94 in 2005-2009 and 5.45 in 2010-2013) and HFrEF (women: 4.78 in 2005-2009 to 5.14 in 2010-2013; men: 4.62 in 2005-2009 and 5.06 in 2010-2013; P-trend<0.0001 for all). Higher comorbidity burden was significantly associated with higher adjusted risk of 1-year mortality, with a stronger association noted for HFpEF (hazard ratio [HR] per 1 higher comorbidity, 1.19 [95% CI, 1.14-1.25] versus HFrEF (HR, 1.10 [95% CI, 1.05-1.14]; P for interaction by HF type=0.02). The associated mortality risk per 1 higher comorbidity also increased significantly over time for patients with HFpEF and HFrEF, as well (P for interaction with time=0.002 and 0.02, respectively) Conclusions: The burden of comorbidities among hospitalized patients with acute decompensated HFpEF and HFrEF has increased over time, as has its associated mortality risk. Higher burden of comorbidities is associated with higher risk of mortality, with a stronger association noted among patients with HFpEF versus HFrEF.
Keywords: comorbidity; heart failure; mortality.
Figures
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS, American Heart Association Council on E, Prevention Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019;139:e56–e528. - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Pina IL, Trogdon JG, American Heart Association Advocacy Coordinating C, Council on Arteriosclerosis T, Vascular B, Council on Cardiovascular R, Intervention, Council on Clinical C, Council on E, Prevention and Stroke C. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–19. - PMC - PubMed
-
- Edelmann F, Stahrenberg R, Gelbrich G, Durstewitz K, Angermann CE, Dungen HD, Scheffold T, Zugck C, Maisch B, Regitz-Zagrosek V, Hasenfuss G, Pieske BM and Wachter R. Contribution of comorbidities to functional impairment is higher in heart failure with preserved than with reduced ejection fraction. Clin Res Cardiol. 2011;100:755–64. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- R01 AG045551/AG/NIA NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- U01 HL125511/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
