

Clinical characteristics and organ system involvement in sarcoidosis: comparison of the University of Minnesota Cohort with other cohorts
- PMID: 32487134
- PMCID: PMC7268634
- DOI: 10.1186/s12890-020-01191-x
Clinical characteristics and organ system involvement in sarcoidosis: comparison of the University of Minnesota Cohort with other cohorts
Abstract
Background: Sarcoidosis is a systemic granulomatous disease of unknown etiology. Clinical cohort studies of different populations are important to understand the high variability in clinical presentation and disease course of sarcoidosis. The aim of the study is to evaluate clinical characteristics, including organ involvement, pulmonary function tests, and laboratory parameters, in a sarcoidosis cohort at the University of Minnesota. We compare the organ system involvement of this cohort with other available cohorts.
Methods: We conducted a retrospective data collection and analysis of 187 subjects with biopsy-proven sarcoidosis seen at a tertiary center. Organ system involvement was determined using the WASOG sarcoidosis organ assessment instrument. Clinical phenotype groups were classified using the Genomic Research in Alpha-1 Antitrypsin Deficiency and Sarcoidosis criteria.
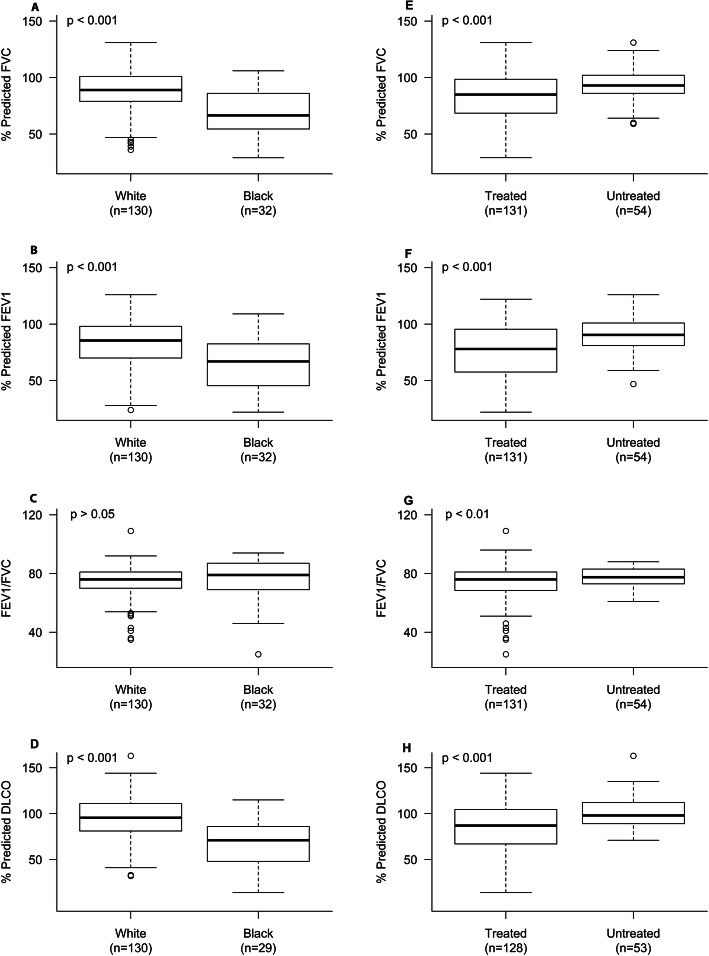
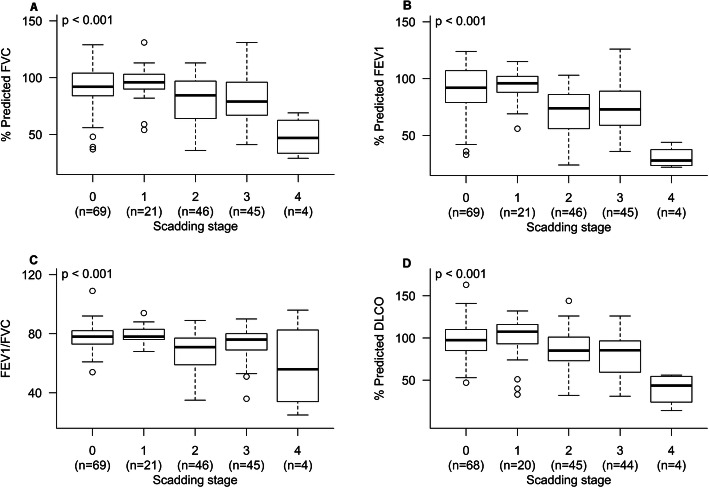
Results: Mean subject age at diagnosis was 45.8 ± 12.4, with a higher proportion of males (55.1%), and a higher proportion of blacks (17.1%) compared to the racial distribution of Minnesota residents (5.95%). The majority (71.1%) of subjects required anti-inflammatory therapy for at least 1 month. Compared to the A Case Control Etiologic Study of Sarcoidosis cohort, there was a higher frequency of extra-thoracic lymph node (34.2% vs. 15.2%), eye (20.9% vs. 11.8%), liver (17.6% vs. 11.5%), spleen (20.9% vs. 6.7%), musculoskeletal (9.6% vs. 0.5%), and cardiac (10.7% vs. 2.3%) involvement in our cohort. A multisystem disease with at least five different organs involved was identified in 13.4% of subjects. A restrictive physiological pattern was observed in 21.6% of subjects, followed by an obstructive pattern in 17.3% and mixed obstructive and restrictive pattern in 2.2%. Almost half (49.2%) were Scadding stages II/III. Commonly employed disease activity markers, including soluble interleukin-2 receptor and angiotensin-converting enzyme, did not differ between treated and untreated groups.
Conclusions: This cohort features a relatively high frequency of high-risk sarcoidosis phenotypes including cardiac and multiorgan disease. Commonly-utilized serum biomarkers do not identify subpopulations that require or do better with treatment. Findings from this study further highlight the high-variability nature of sarcoidosis and the need for a more reliable biomarker to predict and measure disease severity and outcomes for better clinical management of sarcoidosis patients.
Keywords: Clinical characteristics; Clinical phenotyping; Cohort; Organ system involvement; Sarcoidosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999;160(2):736–55. - PubMed
-
- Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet PY, Muller-Quernheim J. Sarcoidosis. Lancet. 2014;383(9923):1155–1167. - PubMed
-
- Erdal BS, Clymer BD, Yildiz VO, Julian MW, Crouser ED. Unexpectedly high prevalence of sarcoidosis in a representative U.S. metropolitan population. Respir Med. 2012;106(6):893–899. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
