

Progressive supranuclear palsy: Advances in diagnosis and management
- PMID: 32487421
- PMCID: PMC7462164
- DOI: 10.1016/j.parkreldis.2020.04.014
Progressive supranuclear palsy: Advances in diagnosis and management
Abstract
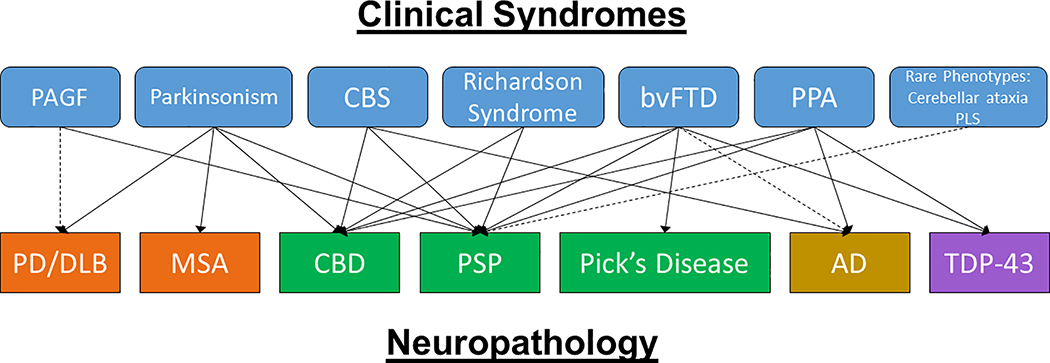
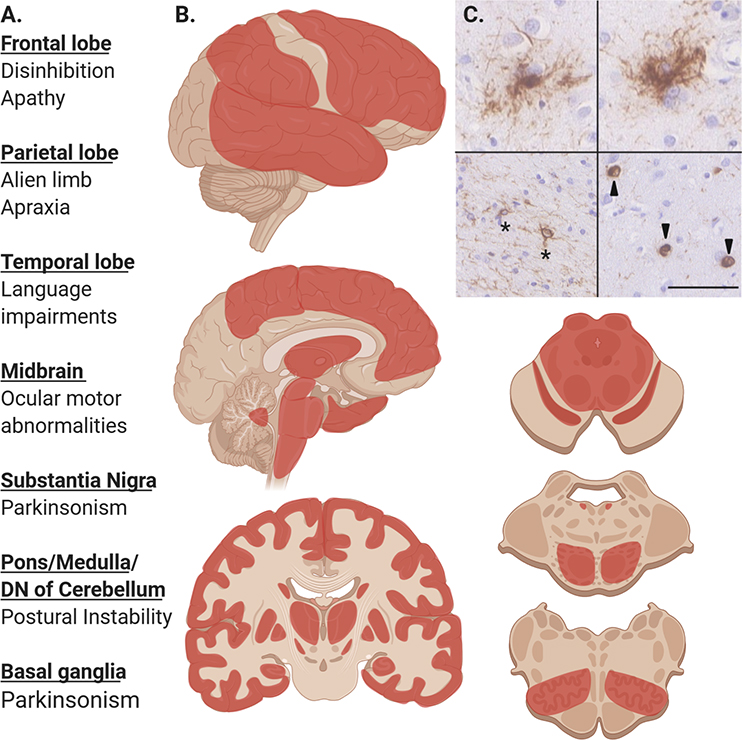
Progressive supranuclear palsy (PSP) is a complex clinicopathologic disease with no current cure or disease modulating therapies that can only be definitively confirmed at autopsy. Growing understanding of the phenotypic diversity of PSP has led to expanded clinical criteria and new insights into etiopathogenesis that coupled with improved in vivo biomarkers makes increased access to current clinical trials possible. Current standard-of-care treatment of PSP is multidisciplinary, supportive and symptomatic, and several trials of potentially disease modulating agents have already been completed with disappointing results. Current ongoing clinical trials target the abnormal aggregation of tau through a variety of mechanisms including immunotherapy and gene therapy offer a more direct method of treatment. Here we review PSP clinicopathologic correlations, in vivo biomarkers including MRI, PET, and CSF biomarkers. We additionally review current pharmacologic and non-pharmacologic methods of treatment, prior and ongoing clinical trials in PSP. Newly expanded clinical criteria and improved specific biomarkers will aid in identifying patients with PSP earlier and more accurately and expand access to these potentially beneficial clinical trials.
Keywords: Gene therapy; Immunotherapy; Progressive supranuclear palsy; Tauopathy; Treatment.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Dr. Coughlin has no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Dr. Litvan’s research is supported in part by Parkinson Study Group, Michael J Fox Foundation, Parkinson Foundation, Lewy Body Association, Roche, Abbvie, Biogen, EIP-Pharma and Biohaven Pharmaceuticals. She was member of a Lundbeck Advisory Board and participated in a symposium organized by Sunovion.
Figures
References
-
- Steele JC, Richardson JC, Olszewski J, PROGRESSIVE SUPRANUCLEAR PALSY. A HETEROGENEOUS DEGENERATION INVOLVING THE BRAIN STEM, BASAL GANGLIA AND CEREBELLUM WITH VERTICAL GAZE AND PSEUDOBULBAR PALSY, NUCHAL DYSTONIA AND DEMENTIA, Arch. Neurol. 10 (1964) 333–59. - PubMed
-
- Hauw J-J, Daniel S, Dickson D, Horoupian D, Jellinger K, Lantos P, McKee A, Tabaton M, Litvan I, Preliminary NINDS neuropathologic criteria for Steele‐Richardson‐Olszewski syndrome (progressive supranuclear palsy), Neurology 44(11) (1994) 2015–2015. - PubMed
-
- Goedert M, Spillantini M, Cairns N, Crowther R, Tau proteins of Alzheimer paired helical filaments: abnormal phosphorylation of all six brain isoforms, Neuron 8(1) (1992) 159–168. - PubMed
-
- Greenberg S, Davies P, Schein J, Binder L, Hydrofluoric acid-treated tau PHF proteins display the same biochemical properties as normal tau, J. Biol. Chem. 267(1) (1992) 564–569. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
