

Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children
- PMID: 32488505
- PMCID: PMC7266128
- DOI: 10.1186/s13613-020-00690-8
Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children
Abstract
Background: A recent increase in children admitted with hypotensive shock and fever in the context of the COVID-19 outbreak requires an urgent characterization and assessment of the involvement of SARS-CoV-2 infection. This is a case series performed at 4 academic tertiary care centers in Paris of all the children admitted to the pediatric intensive care unit (PICU) with shock, fever and suspected SARS-CoV-2 infection between April 15th and April 27th, 2020.
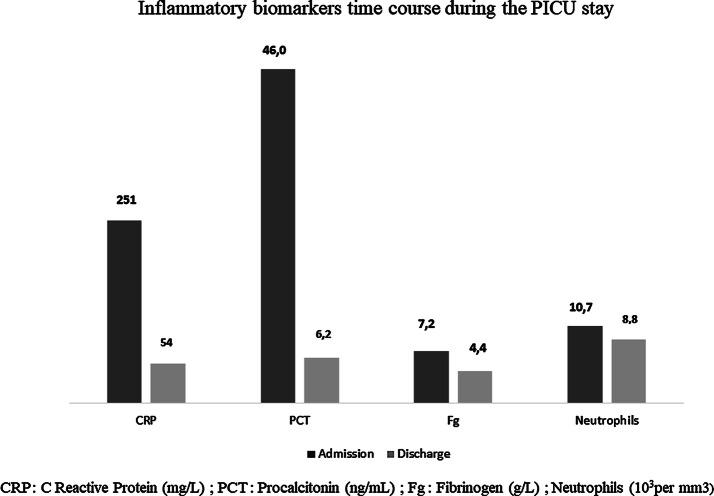
Results: 20 critically ill children admitted for shock had an acute myocarditis (left ventricular ejection fraction, 35% (25-55); troponin, 269 ng/mL (31-4607)), and arterial hypotension with mainly vasoplegic clinical presentation. The first symptoms before PICU admission were intense abdominal pain and fever for 6 days (1-10). All children had highly elevated C-reactive protein (> 94 mg/L) and procalcitonin (> 1.6 ng/mL) without microbial cause. At least one feature of Kawasaki disease was found in all children (fever, n = 20, skin rash, n = 10; conjunctivitis, n = 6; cheilitis, n = 5; adenitis, n = 2), but none had the typical form. SARS-CoV-2 PCR and serology were positive for 10 and 15 children, respectively. One child had both negative SARS-CoV-2 PCR and serology, but had a typical SARS-CoV-2 chest tomography scan. All children but one needed an inotropic/vasoactive drug support (epinephrine, n = 12; milrinone, n = 10; dobutamine, n = 6, norepinephrine, n = 4) and 8 were intubated. All children received intravenous immunoglobulin (2 g per kilogram) with adjuvant corticosteroids (n = 2), IL 1 receptor antagonist (n = 1) or a monoclonal antibody against IL-6 receptor (n = 1). All children survived and were afebrile with a full left ventricular function recovery at PICU discharge.
Conclusions: Acute myocarditis with intense systemic inflammation and atypical Kawasaki disease is an emerging severe pediatric disease following SARS-CoV-2 infection. Early recognition of this disease is needed and referral to an expert center is recommended. A delayed and inappropriate host immunological response is suspected. While underlying mechanisms remain unclear, further investigations are required to target an optimal treatment.
Keywords: Acute myocarditis; Children; Multisystem inflammatory syndrome; SARS-CoV-2; Shock.
Conflict of interest statement
No.
Figures
References
-
- Tagarro A, Epalza C, Santos M, Sanz-Santaeufemia FJ, Otheo E, Moraleda C, et al. Screening and severity of coronavirus disease 2019 (COVID-19) in Children in Madrid, Spain. JAMA Pediatr. 2020. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2764394 Accessed 12 Apr 2020. - PMC - PubMed
-
- Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr. 2020;. - PubMed
-
- Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, Tomasoni D, et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020. https://jamanetwork.com/journals/jamacardiology/fullarticle/2763843 Accessed 7 May 2020. - PMC - PubMed
-
- Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020. https://jamanetwork.com/journals/jamacardiology/fullarticle/2763846 Accessed 7 May 2020. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
