

Ultra rapid lispro improves postprandial glucose control compared with lispro in patients with type 1 diabetes: Results from the 26-week PRONTO-T1D study
- PMID: 32488923
- PMCID: PMC7539952
- DOI: 10.1111/dom.14100
Ultra rapid lispro improves postprandial glucose control compared with lispro in patients with type 1 diabetes: Results from the 26-week PRONTO-T1D study
Abstract
Aims: To evaluate the efficacy and safety of ultra rapid lispro (URLi) versus lispro in adults with type 1 diabetes in a 26-week, treat-to-target, phase 3 trial.
Materials and methods: After an 8-week lead-in to optimize basal insulin glargine or degludec, patients were randomized to double-blind mealtime URLi (n = 451) or lispro (n = 442), or open-label post-meal URLi (n = 329). The primary endpoint was change from baseline glycated haemoglobin (HbA1c) to 26 weeks (non-inferiority margin 0.4%), with multiplicity-adjusted objectives for postprandial glucose (PPG) excursions after a meal test.
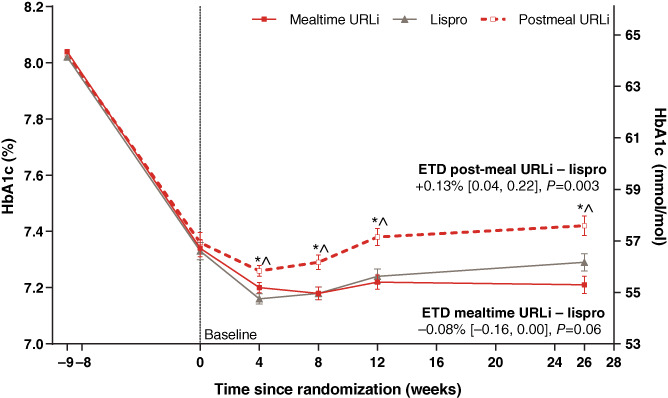
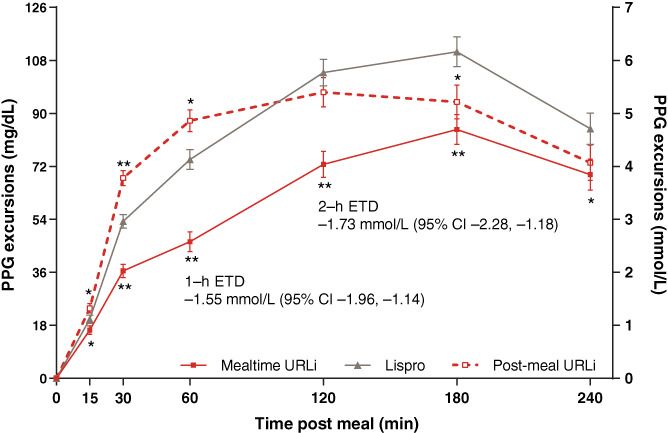
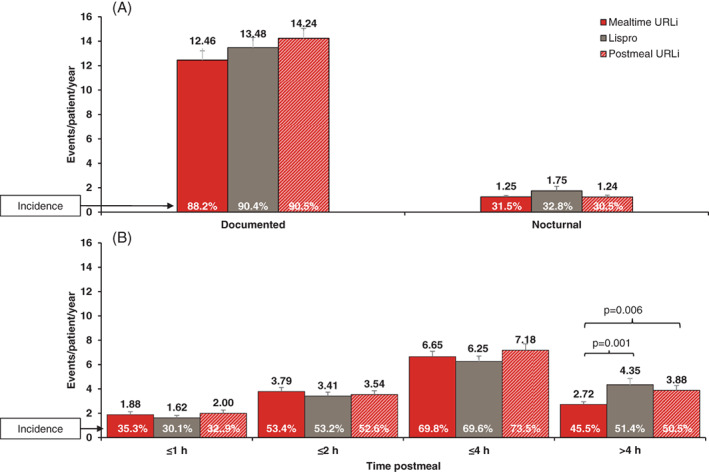
Results: Both mealtime and post-meal URLi demonstrated non-inferiority to lispro for HbA1c: estimated treatment difference (ETD) for mealtime URLi -0.08% [95% confidence interval (CI) -0.16, 0.00] and for post-meal URLi +0.13% (95% CI 0.04, 0.22), with a significantly higher endpoint HbA1c for post-meal URLi versus lispro (P = 0.003). Mealtime URLi was superior to lispro in reducing 1- and 2-hour PPG excursions during the meal test: ETD -1.55 mmol/L (95% CI -1.96, -1.14) at 1 hour and - 1.73 mmol/L (95% CI -2.28, -1.18) at 2 hours (both P < 0.001). The rate and incidence of severe, documented and postprandial hypoglycaemia (<3.0 mmol/L) was similar between treatments, but mealtime URLi demonstrated a 37% lower rate in the period >4 hours after meals (P = 0.013). Injection site reactions were reported by 2.9% of patients on mealtime URLi, 2.4% on post-meal URLi, and 0.2% on lispro. Overall, the incidence of treatment-emergent adverse events was similar between treatments.
Conclusions: The results showed that URLi provided good glycaemic control, with non-inferiority to lispro confirmed for both mealtime and post-meal URLi, while superior PPG control was demonstrated with mealtime dosing.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
L.K. received research grants from Abbott, Ascensia Diabetes Care, Cnoga Medical, Eli Lilly and Company, Gan & Lee, Medtronic, Novo Nordisk, REMD Biotherapeutics, Sanofi, Senseonics, Xeris and Zealand Pharma. D.C., M.A.D., J.T. and J.M.B‐V. are employees and shareholders of Eli Lilly and Company. J.M. received speaker fees from Abbott, Astellas, Astra Zeneca, Böhringer Ingelheim, Eli Lilly and Company, Johnson & Johnson, Kyowa Kirin, Novartis, Novo Nordisk, MSD, Mylan, Taisho Pharma, Tanabe‐Mitsubishi, Terumo and Sanofi, and consultant fees from Abbott, Astra Zeneca, Kanro, Kowa, and Terumo. D.D. received research grants or speaker fees from Astra Zeneca, Böhringer Ingelheim, Eli Lilly and Company, Lexicon Pharma, Mylan, Novartis, Novo Nordisk, and Zealand Pharma. J.L reports no conflicts of interest. No other potential conflicts of interest relevant to this article were reported.
Figures
References
-
- Ceriello A. Postprandial hyperglycemia and diabetes complications: is it time to treat? Diabetes. 2005;54(1):1‐7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
