

A randomised evaluation of intercostal block as an adjunct to epidural analgesia for post-thoracotomy pain
- PMID: 32489201
- PMCID: PMC7259421
- DOI: 10.4103/ija.IJA_714_19
A randomised evaluation of intercostal block as an adjunct to epidural analgesia for post-thoracotomy pain
Abstract
Background and aims: Post-thoracotomy pain can be severe and disabling. The aim of this study was to examine the efficacy of intercostal nerve block when used as adjunct to thoracic epidural analgesia in patients undergoing posterolateral thoracotomy.
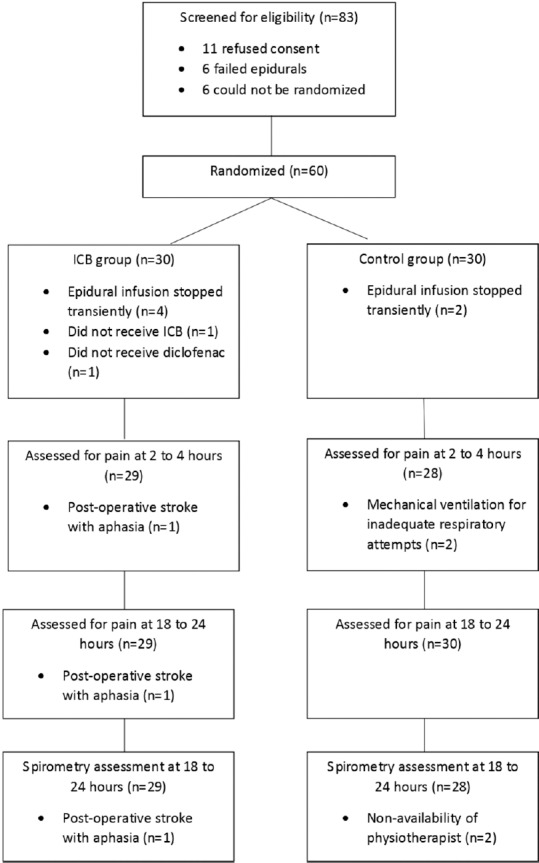
Methods: This was a parallel-group randomised patient and assessor-blinded study carried out at a tertiary-referral cancer center. We included 60 adult patients undergoing elective lung resection under general anaesthesia with thoracic epidural analgesia. In addition, the intervention arm received single-shot intercostal blocks with 10 ml of 0.25% bupivacaine at the level of and two levels above and below the thoracotomy. We assessed post-operative pain scores at 2 to 4 hours and 18 to 24 hours after surgery, peri-operative fentanyl requirement, percentage of patients who needed fentanyl PCA and maximum volume achieved on bedside spirometry 18 to 24 hours after surgery. Groups were compared using the unpaired t-test for continuous data and the chi square test for categorical data at a 5% level of significance.
Results: 2 to 4 hours post-operatively, mean pain scores at rest were 3.0 in both groups (difference 0.04, 95% CI -1.1 to + 1.1) and on coughing were 4.6 (ICB group) and 4.9 (C group) (difference 0.32, 95% CI -1.0 to + 1.6). There were no differences between the groups for any of the other outcomes.
Conclusion: Addition of intercostal block to epidural analgesia does not confer any benefit in terms of post-operative pain, fentanyl requirements or volume achieved on spirometry.
Keywords: Analgesia; epidural; intercostal nerve; thoracotomy.
Copyright: © 2020 Indian Journal of Anaesthesia.
Conflict of interest statement
There are no conflicts of interest.
References
-
- Prospect – Procedure specific post-operative pain management. [Internet] [Last cited on 2018 Dec 17]. Available from: http://www.postoppain.org/frameset.htm .
-
- De Cosmo G, Aceto P, Gualtieri E, Congedo E. Analgesia in thoracic surgery: Review. Minerva Anestesiol. 2009;75:393–400. - PubMed
-
- Hermanides J, Hollmann MW, Stevens MF, Lirk P. Failed epidural: Causes and management. Br J Anaesth. 2012;109:144–54. - PubMed
-
- Takamori S, Yoshida S, Hayashi A, Matsuo T, Mitsuoka M, Shirouzu K. Intraoperative intercostal nerve blockade for postthoracotomy pain. Ann Thorac Surg. 2002;74:338–41. - PubMed
-
- Concha M, Dagnino J, Cariaga M, Aguilera J, Aparicio R, Guerrero M. Analgesia after thoracotomy: Epidural fentanyl/bupivacaine compared with intercostal nerve block plus intravenous morphine. J Cardiothorac Vasc Anesth. 2004;18:322–6. - PubMed
LinkOut - more resources
Full Text Sources