

Canadian consensus: a new systemic treatment algorithm for advanced EGFR- mutated non-small-cell lung cancer
- PMID: 32489263
- PMCID: PMC7253730
- DOI: 10.3747/co.27.6007
Canadian consensus: a new systemic treatment algorithm for advanced EGFR- mutated non-small-cell lung cancer
Abstract
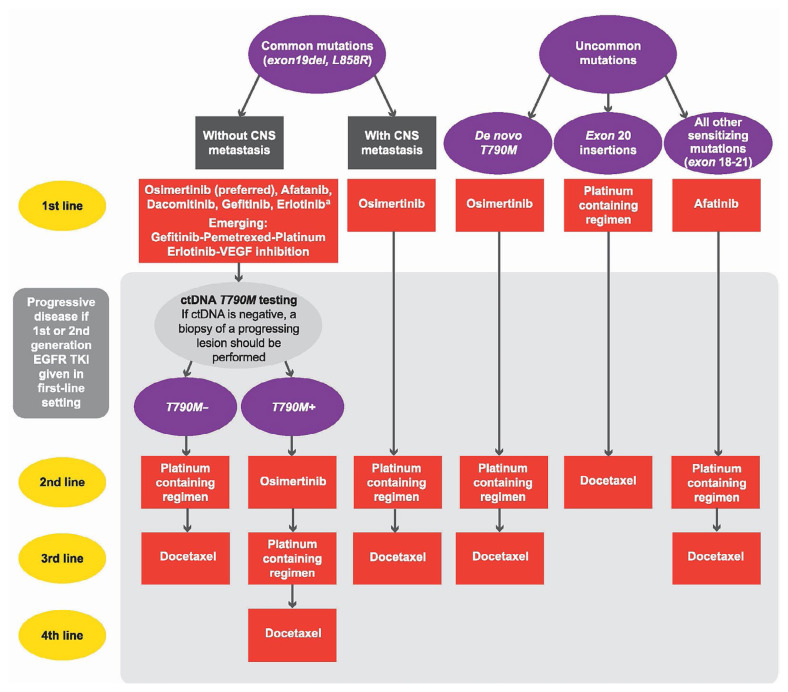
Background: Multiple clinical trials for the treatment of advanced EGFR-mutated non-small-cell lung cancer (nsclc) have recently been reported. As a result, the treatment algorithm has changed, and many important clinical questions have been raised:■ What is the optimal first-line treatment for patients with EGFR-mutated nsclc?■ What is preferred first-line treatment for patients with brain metastasis?■ What is the preferred second-line treatment for patients who received first-line first- or second-generation tyrosine kinase inhibitors (tkis)?■ What is the preferred treatment after osimertinib?■ What evidence do we have for treating patients whose tumours harbour uncommon EGFR mutations?
Methods: A Canadian expert panel was convened to define the key clinical questions, review recent evidence, and discuss and agree on practice recommendations for the treatment of advanced EGFR-mutated nsclc.
Results: The published overall survival results for osimertinib, combined with its central nervous system activity, have led to osimertinib becoming the preferred first-line treatment for patients with common EGFR mutations, including those with brain metastasis. Other agents could still have a role, especially when osimertinib is not available or not tolerated. Treatment in subsequent lines of therapy depends on the first-line therapy or on T790M mutation status. Treatment recommendations for patients whose tumours harbour uncommon EGFR mutations are guided mainly by retrospective and limited prospective evidence. Finally, the evidence for sequencing and combining tkis with chemotherapy, angiogenesis inhibitors, checkpoint inhibitors, and other new therapeutics is reviewed.
Conclusions: This Canadian expert consensus statement and algorithm were driven by significant advances in the treatment of EGFR-mutated nsclc.
Keywords: EGFR mutation; Non-small-cell lung cancer, advanced; acquired resistance; algorithms; mutations, common; mutations, uncommon; nsclc; sequencing.
2020 Multimed Inc.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES We have read and understood Current Oncology’s policy on disclosing conflicts of interest, and we declare the following interests: BM has received honoraria for advisory board participation from Bayer, Pfizer, AstraZeneca, Boehringer Ingelheim, and Roche. SB has received honoraria for advisory board participation from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol–Myers Squibb, GlaxoSmithKline, Lilly, Merck, Novartis, Pfizer, Roche, and Takeda. NB has received honoraria for advisory board participation from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol–Myers Squibb, GlaxoSmithKline, Lilly, Merck, Novartis, Pfizer, Roche, and Takeda, and has received research funding from AstraZeneca. QC has received honoraria for advisory board participation from AbbVie, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol–Myers Squibb, Eisai, Eli Lilly, Merck, Novartis, Pfizer, Roche, and Takeda. RJ has received honoraria for advisory board participation from AstraZeneca, Bristol–Myers Squibb, Fusion, Merck, Novartis, Pfizer, Roche, and Takeda, and research funding from AstraZeneca, Bristol–Myers Squibb, and Merck. NBL is a beneficiary of institutional research funding from Guardant, Array, Novartis, Merck, and Roche; has received honoraria or travel expenses for independent continuing medical education from Roche, AstraZeneca, Merck Sharp and Dohme, and Bristol–Myers Squibb; and has acted as an advisor (compensated) for Xcovery and as a consultant for the Canadian Agency for Drugs and Technologies in Health. GL has received honoraria for advisory board participation from AstraZeneca, Roche, Pfizer, Takeda, Novartis, Merck, Bristol–Myers Squibb, Boehringer Ingelheim, and Bayer, and for providing education consulting services to AstraZeneca, Roche, emd Serono, and Takeda. GL has also received research funding from AstraZeneca, Roche, and Takeda. PC has received honoraria for advisory board participation from AstraZeneca, Boehringer Ingelheim, Roche, Pfizer, Takeda, Merck, and Bristol–Myers Squibb.
Figures
References
-
- Rosell R, Carcereny E, Gervais R, et al. on behalf of the Spanish Lung Cancer Group in collaboration with the Groupe français de pneumo-cancérologie and the Associazione Italiana Oncologia Toracica. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation–positive non-small-cell lung cancer (eurtac): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–46. doi: 10.1016/S1470-2045(11)70393-X. - DOI - PubMed
-
- Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation–positive non-small-cell lung cancer (optimal, ctong-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–42. doi: 10.1016/S1470-2045(11)70184-X. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
