

Fluid management and deresuscitation practices: A survey of critical care physicians
- PMID: 32489406
- PMCID: PMC7238475
- DOI: 10.1177/1751143719846442
Fluid management and deresuscitation practices: A survey of critical care physicians
Abstract
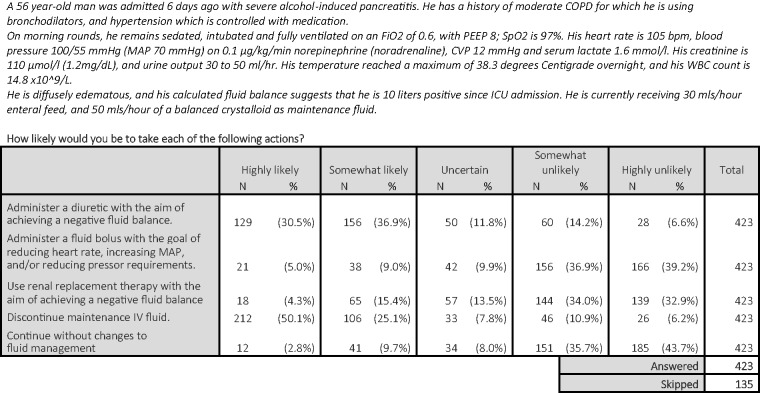
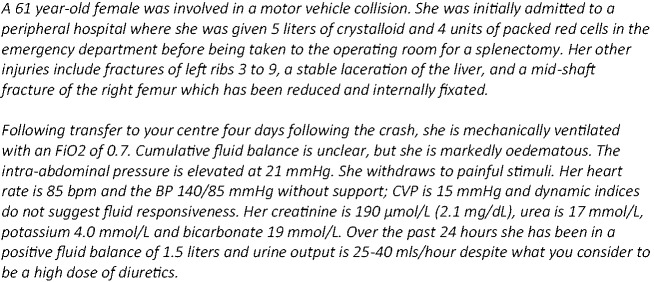
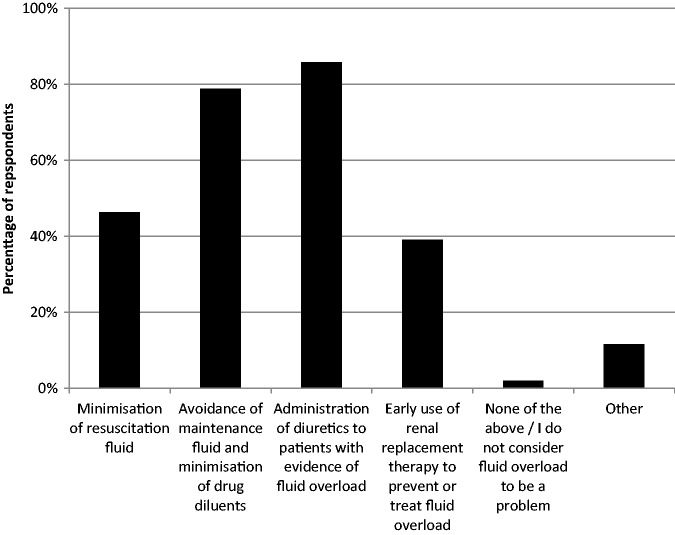
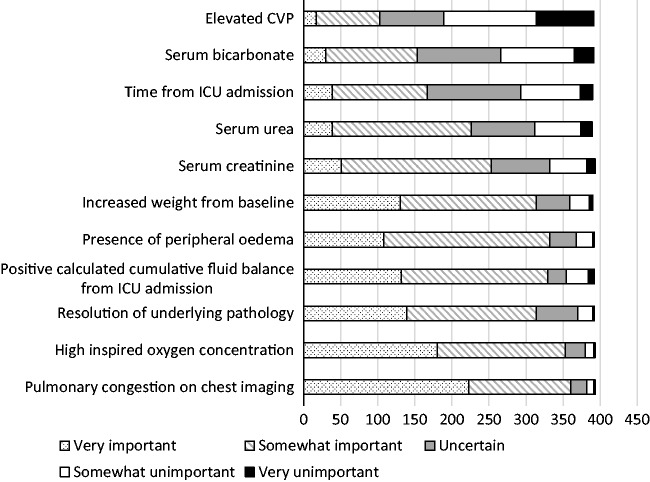
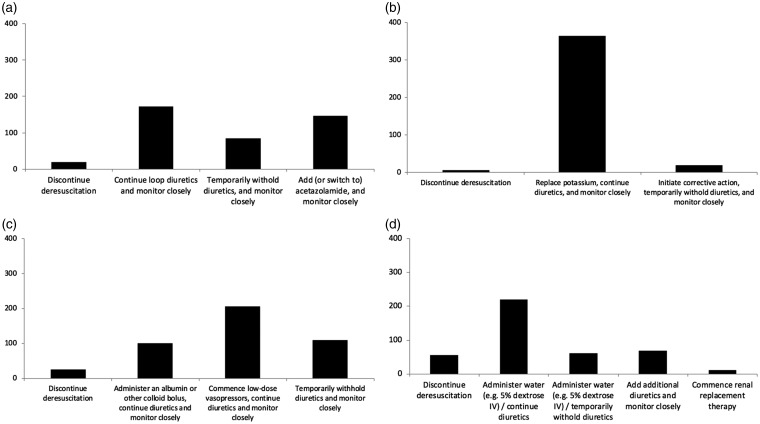
Accumulation of a positive fluid balance is common in critically ill patients, and is associated with adverse outcomes, including mortality. However, there are few randomised clinical trials to guide clinicians as to the most appropriate fluid strategy following initial resuscitation and on the use of deresuscitation (removal of accumulated fluid using diuretics and/or renal replacement therapy). To inform the design of randomised trials, we surveyed critical care physicians with regard to perceptions of fluid overload in critical care, self-reported practice, acceptability of a variety of approaches to deresuscitation, appropriate safety parameters, and overall acceptability of a randomised trial of deresuscitation. Of 524 critical care specialists completing the survey, the majority practiced in mixed medical/surgical intensive care units in the United Kingdom. Most (309 of 363 respondents, 85%) believed fluid overload to be a modifiable source of morbidity; there was strong support (395 of 457, 86%) for a randomised trial of deresuscitation in critical illness. Marked practice variability was evident among respondents. In a given clinical scenario, self-reported practice ranged from the administration of fluid (N = 59, 14%) to the administration of a diuretic (N = 285, 67%). The majority (95%) considered it appropriate to administer diuretics for fluid overload in the setting of noradrenaline infusion and to continue to administer diuretics despite mild dysnatraemias, hypotension, metabolic alkalosis, and hypokalaemia. The majority of critical care physicians view fluid overload as a common and modifiable source of morbidity; deresuscitation is widely practiced, and there is widespread support for randomised trials of deresuscitation in critical illness.
Keywords: Critical illness; critical care; deresuscitation; diuretics; fluid therapy; water–electrolyte balance.
© The Intensive Care Society 2019.
Figures
References
-
- Silversides JA, Fitzgerald E, Manickavasagam US, et al. Deresuscitation of patients with iatrogenic fluid overload is associated with reduced mortality in critical illness. Crit Care Med 2018; 46: 1600–1607. - PubMed
-
- Murphy CV, Schramm GE, Doherty JA, et al. The importance of fluid management in acute lung injury secondary to septic shock. Chest 2009; 136: 102–109. - PubMed
LinkOut - more resources
Full Text Sources