

Hypoglycaemia and cardiac arrhythmias in diabetes
- PMID: 32489579
- PMCID: PMC7238305
- DOI: 10.1177/2042018820911803
Hypoglycaemia and cardiac arrhythmias in diabetes
Abstract
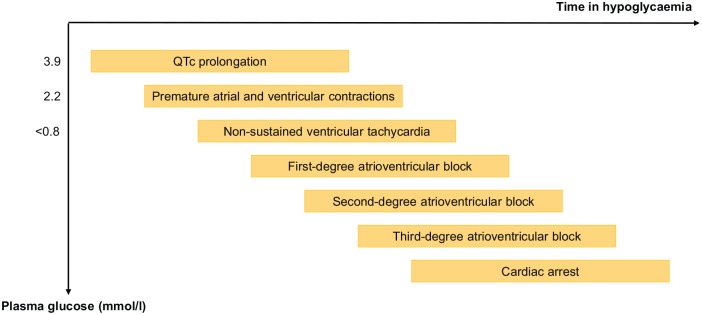
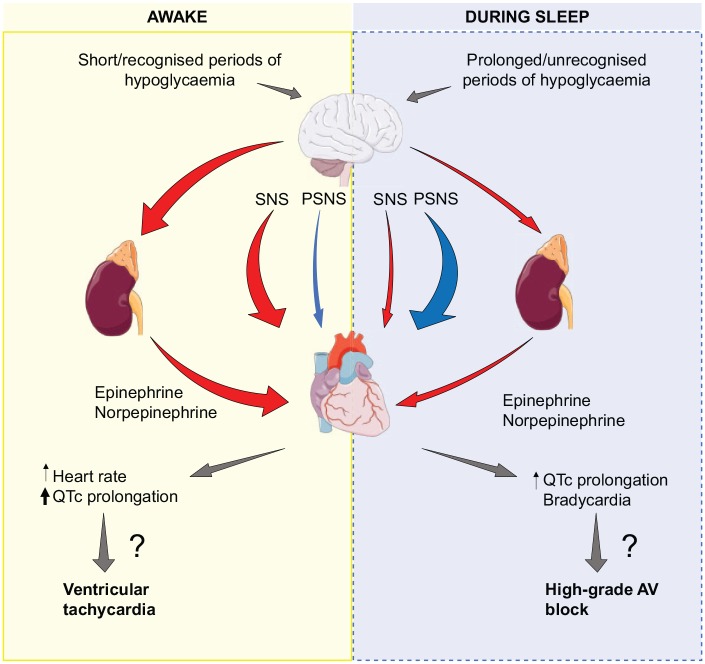
Hypoglycaemia remains an inevitable risk in insulin-treated type 1 diabetes and type 2 diabetes and has been associated with multiple adverse outcomes. Whether hypoglycaemia is a cause of fatal cardiac arrhythmias in diabetes, or merely a marker of vulnerability, is still unknown. Since a pivotal report in 1991, hypoglycaemia has been suspected to induce cardiac arrhythmias in patients with type 1 diabetes, the so-called 'dead-in-bed syndrome'. This suspicion has subsequently been supported by the coexistence of an increased mortality and a three-fold increase in severe hypoglycaemia in patients with type 2 diabetes receiving intensive glucose-lowering treatment in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Studies have investigated the association between hypoglycaemia-induced cardiac arrhythmias. In a rat-model, severe hypoglycaemia resulted in a specific pattern of cardiac arrhythmias including QT-prolongation, ventricular tachycardia, second- and third-degree AV block and ultimately cardiorespiratory arrest. In clinical studies of experimentally induced hypoglycaemia, QTc-prolongation, a risk factor of ventricular arrhythmias, is an almost consistent finding. The extent of QT-prolongation seems to be modified by several factors, including antecedent hypoglycaemia, diabetes duration and cardiac autonomic neuropathy. Observational studies indicate diurnal differences in the pattern of electrocardiographic alterations during hypoglycaemia with larger QTc-prolongations during daytime, whereas the risk of bradyarrhythmias may be increased during sleep. Daytime periods of hypoglycaemia are characterized by shorter duration, increased awareness and a larger increase in catecholamines. The counterregulatory response is reduced during nightly episodes of hypoglycaemia, resulting in prolonged periods of hypoglycaemia with multiple nadirs. An initial sympathetic activity at plasma glucose nadir is replaced by increased vagal activity, which results in bradycardia. Here, we provide an overview of the existing literature exploring potential mechanisms for hypoglycaemia-induced cardiac arrhythmias and studies linking hypoglycaemia to cardiac arrhythmias in patients with diabetes.
Keywords: cardiac arrhythmias; diabetes complications; hypoglycaemia; type 1 diabetes; type 2 diabetes.
© The Author(s), 2020.
Conflict of interest statement
Conflicts of interest statement: A.A. has no conflicts of interest. P.G.J. has received lecture fee from Novo Nordisk. F.K.K. has served on scientific advisory panels and been part of speaker’s bureaus for, served as a consultant to or received research support from Amgen, AstraZeneca, Boehringer Ingelheim, Carmot Therapeutics, Eli Lilly, Gubra, Lupin, MedImmune, MSD/Merck, Mundipharma, Norgine, Novo Nordisk, Sanofi and Zealand Pharma. T.V. declares personal fees from Amgen, Boehringer Ingelheim, Eli Lilly, AstraZeneca, Merck Sharp and Dohme, Mundipharma, Sanofi, Sun Pharma, Novo Nordisk and Bristol-Myers Squibb, and grants (to her institution) from Eli Lilly, Boehringer Ingelheim, and Novo Nordisk.
Figures
References
-
- Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352: 854–865. - PubMed
-
- Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008; 359: 1577–1589. - PubMed
-
- Andersen A, Lund A, Knop FK, et al. Glucagon-like peptide 1 in health and disease. Nat Rev Endocrinol 2018; 14: 390–403. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
