

SRμCT Reveals 3D Microstructural Alterations of the Vascular and Neuronal Network in a Rat Model of Chronic Compressive Thoracic Spinal Cord Injury
- PMID: 32489705
- PMCID: PMC7220295
- DOI: 10.14336/AD.2019.0529
SRμCT Reveals 3D Microstructural Alterations of the Vascular and Neuronal Network in a Rat Model of Chronic Compressive Thoracic Spinal Cord Injury
Abstract
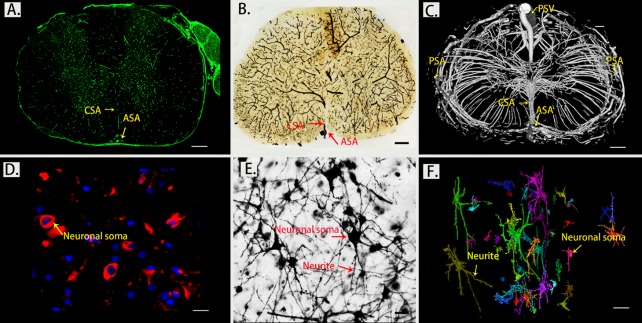
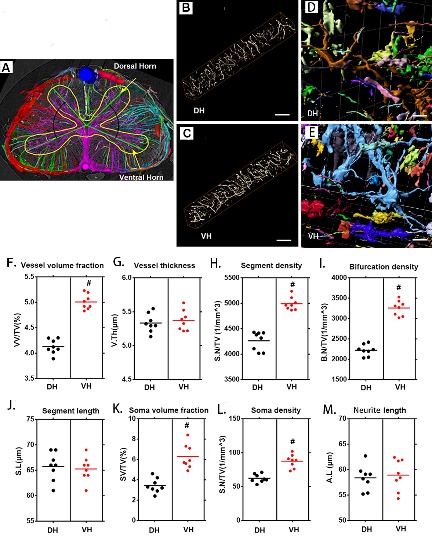
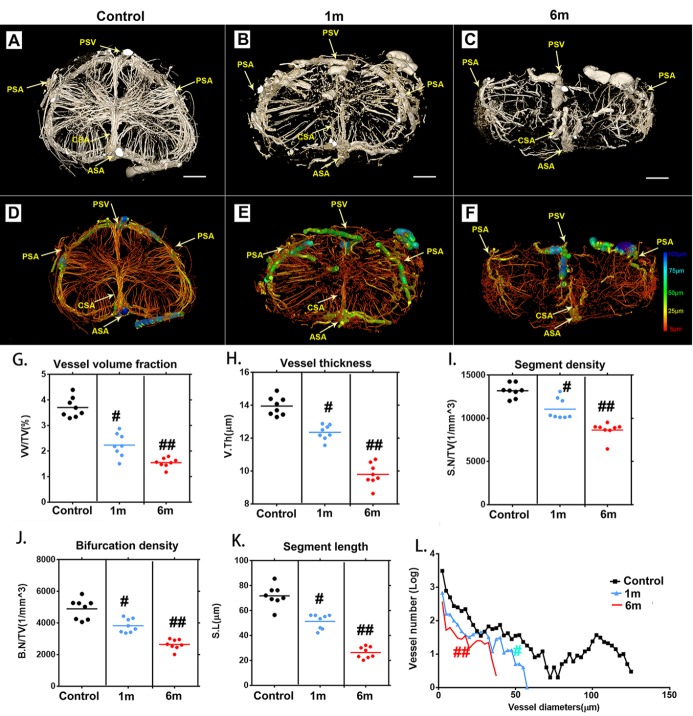
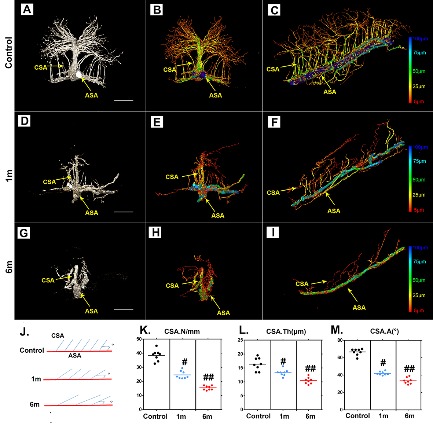
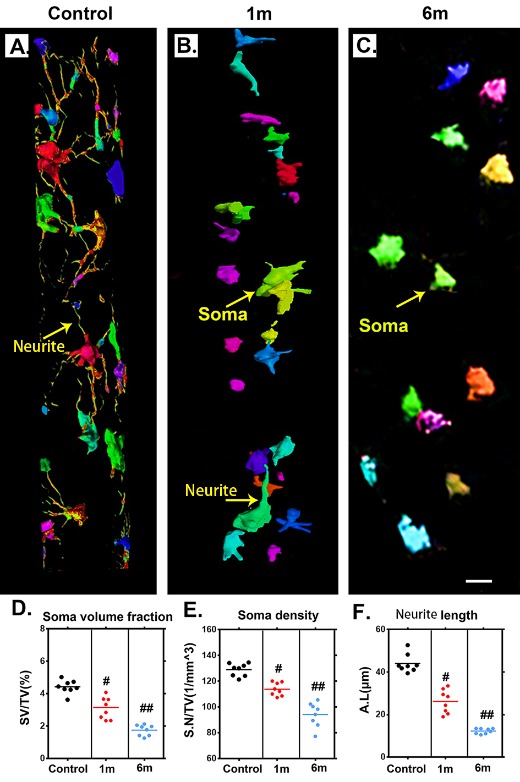
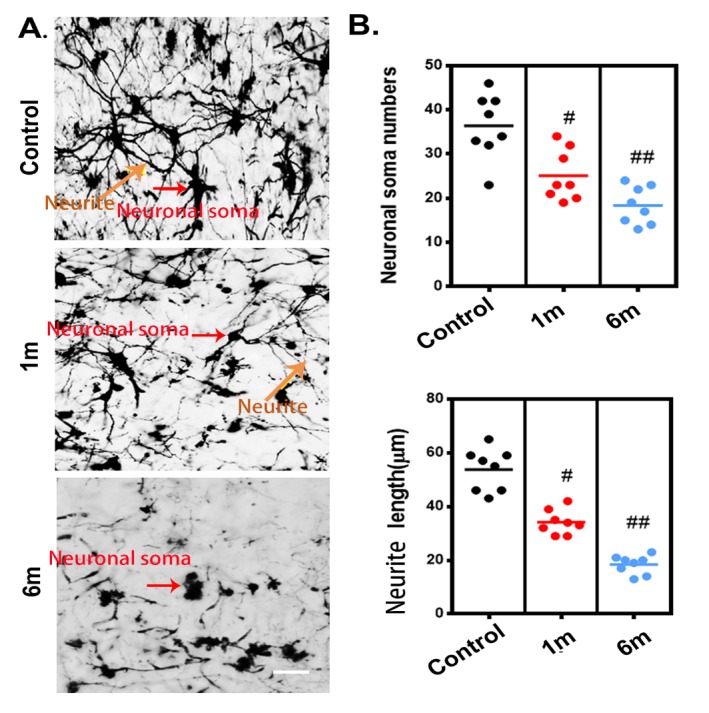
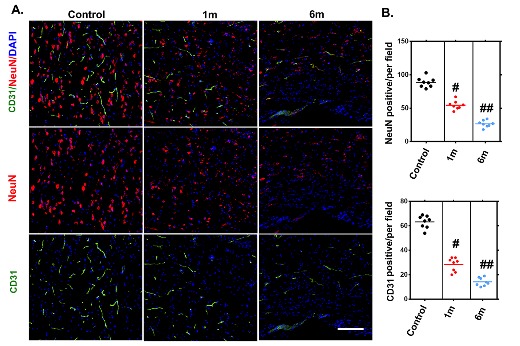
The complex pathology of chronic thoracic spinal cord compression involves vascular and neuroarchitectural repair processes that are still largely unknown. In this study, we used synchrotron radiation microtomography (SRμCT) to quantitatively characterize the 3D temporal-spatial changes in the vascular and neuronal network after chronic thoracic spinal cord compression in order to obtain further insights into the pathogenesis of this disease and to elucidate its underlying mechanisms. Direct 3D characterization of the spinal cord microvasculature and neural microstructure of the thoracic spinal cord was successfully reconstructed. The significant reduction in vasculature and degeneration of neurons in the thoracic spinal cord visualized via SRμCT after chronic compression were consistent with the changes detected by immunofluorescence staining. The 3D morphological measurements revealed significant reductions of neurovascular parameters in the thoracic spinal cord after 1 month of compression and became even worse after 6 months without relief of compression. In addition, the distinct 3D morphological twist and the decrease in branches of the central sulcal artery after chronic compression vividly displayed that these could be the potential triggers leading to blood flow reduction and neural deficits of the thoracic spinal cord. Our findings propose a novel methodology for the 3D analysis of neurovascular repair in chronic spinal cord compression, both qualitatively and quantitatively. The results indicated that compression simultaneously caused vascular dysfunction and neuronal network impairment, which should be acknowledged as concurrent events after chronic thoracic spinal cord injury. Combining neuroprotection with vasoprotection may provide promising therapeutic targets for chronic thoracic spinal cord compression.
Keywords: 3D; SRμCT; chronic spinal cord injury; neurovascular unit; spinal cord microvasculature.
Copyright: © 2020 Jiang et al.
Conflict of interest statement
Disclosure statement No competing financial interests exist.
Figures
References
-
- McKinley WO, Seel RT, Hardman JT (1999). Nontraumatic spinal cord injury: incidence, epidemiology, and functional outcome. Arch Phys Med Rehabil, 80:619-623. - PubMed
-
- Gupta A, Taly AB, Srivastava A, Murali T (2009). Non-traumatic spinal cord lesions: epidemiology, complications, neurological and functional outcome of rehabilitation. Spinal Cord, 47:307-311. - PubMed
-
- New PW, Sundararajan V (2008). Incidence of non-traumatic spinal cord injury in Victoria, Australia: a population-based study and literature review. Spinal Cord, 46:406-411. - PubMed
-
- Maiuri F, Iaconetta G, Gambardella A (2000). Ossification of the yellow ligament causing thoracic cord compression. Arch Orthop Trauma Surg, 120:346-348. - PubMed
LinkOut - more resources
Full Text Sources