

Comorbid Chronic Diseases are Strongly Correlated with Disease Severity among COVID-19 Patients: A Systematic Review and Meta-Analysis
- PMID: 32489711
- PMCID: PMC7220287
- DOI: 10.14336/AD.2020.0502
Comorbid Chronic Diseases are Strongly Correlated with Disease Severity among COVID-19 Patients: A Systematic Review and Meta-Analysis
Abstract
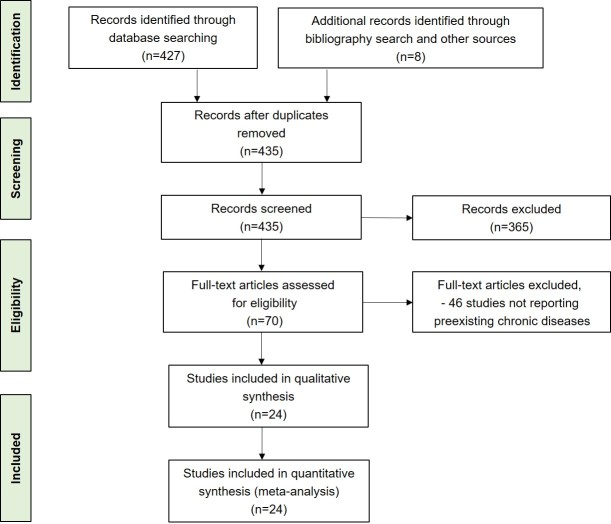
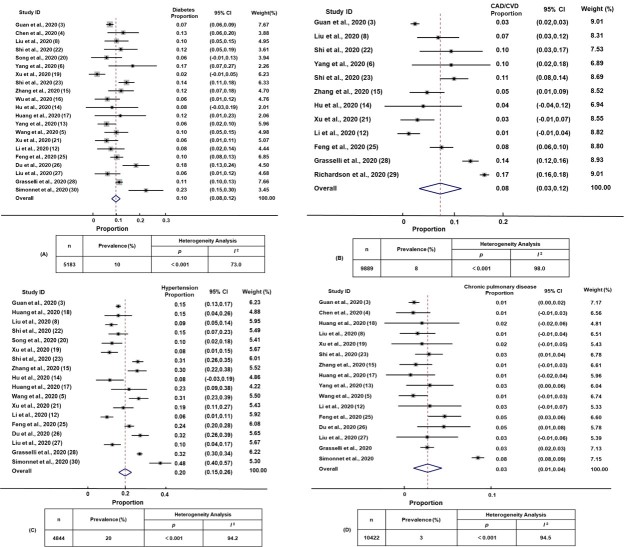
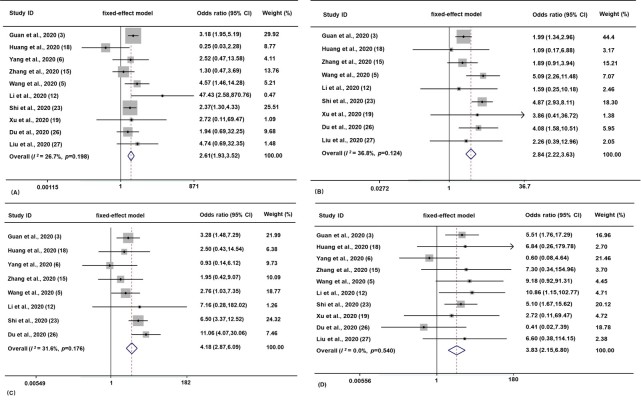
Coronavirus disease 2019 (COVID-19) has resulted in considerable morbidity and mortality worldwide since December 2019. In order to explore the effects of comorbid chronic diseases on clinical outcomes of COVID-19, a search was conducted in PubMed, Ovid MEDLINE, EMBASE, CDC, and NIH databases to April 25, 2020. A total of 24 peer-reviewed articles, including 10948 COVID-19 cases were selected. We found diabetes was present in 10.0%, coronary artery disease/cardiovascular disease (CAD/CVD) was in 8.0%, and hypertension was in 20.0%, which were much higher than that of chronic pulmonary disease (3.0%). Specifically, preexisting chronic conditions are strongly correlated with disease severity [Odds ratio (OR) 3.50, 95% CI 1.78 to 6.90], and being admitted to intensive care unit (ICU) (OR 3.36, 95% CI 1.67 to 6.76); in addition, compared to COVID-19 patients with no preexisting chronic diseases, COVID-19 patients who present with either diabetes, hypertension, CAD/CVD, or chronic pulmonary disease have a higher risk of developing severe disease, with an OR of 2.61 (95% CI 1.93 to 3.52), 2.84 (95% CI 2.22 to 3.63), 4.18 (95% CI 2.87 to 6.09) and 3.83 (95% CI 2.15 to 6.80), respectively. Surprisingly, we found no correlation between chronic conditions and increased risk of mortality (OR 2.09, 95% CI 0.26 to16.67). Taken together, cardio-metabolic diseases, such as diabetes, hypertension and CAD/CVD were more common than chronic pulmonary disease in COVID-19 patients, however, each comorbid disease was correlated with increased disease severity. After active treatment, increased risk of mortality in patients with preexisting chronic diseases may reduce.
Keywords: cardiovascular diseases; chronic pulmonary disease; coronavirus disease 2019 (COVID-19); diabetes; hypertension; meta-analysis.
Copyright: © 2020 Liu et al.
Conflict of interest statement
Conflict of Interest The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous