

High Poverty and Hardship Financing Among Patients with Noncommunicable Diseases in Rural Haiti
- PMID: 32489780
- PMCID: PMC7218772
- DOI: 10.5334/gh.388
High Poverty and Hardship Financing Among Patients with Noncommunicable Diseases in Rural Haiti
Abstract
Background: Poverty is a major barrier to healthcare access in low-income countries. The degree of equitable access for noncommunicable disease (NCD) patients is not known in rural Haiti.
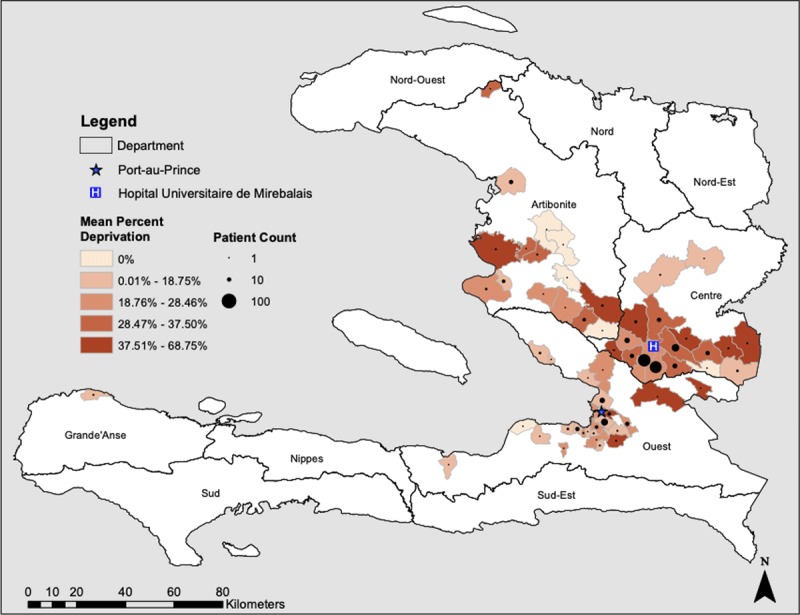
Objectives: We evaluated the poverty distribution among patients receiving care in an NCD clinic in rural Haiti compared with the community and assessed associations of poverty with sex and distance from the health facility.
Methods: We performed a cross-sectional study of patients with NCDs attending a public-sector health center in rural Haiti 2013-2016, and compared poverty among patients with poverty among a weighted community sample from the Haiti 2012 Demographic and Health Survey. We adapted the multidimensional poverty index: people deprived ≥44% of indicators are among the poorest billion people worldwide. We assessed hardship financing: borrowing money or selling belongings to pay for healthcare. We examined the association between facility distance and poverty adjusted for age and sex using linear regression.
Results: Of 379 adults, 72% were women and the mean age was 52.5 years. 17.7% had hypertension, 19.3% had diabetes, 3.1% had heart failure, and 33.8% had multiple conditions. Among patients with available data, 197/296 (66.6%) experienced hardship financing. The proportions of people who are among the poorest billion people for women and men were similar (23.3% vs. 20.3%, p > 0.05). Fewer of the clinic patients were among the poorest billion people compared with the community (22.4% vs. 63.1%, p < 0.001). Patients who were most poor were more likely to live closer to the clinic (p = 0.002).
Conclusion: Among patients with NCD conditions in rural Haiti, poverty and hardship financing are highly prevalent. However, clinic patients were less poor compared with the community population. These data suggest barriers to care access particularly affect the poorest. Socioeconomic data must be collected at health facilities and during community-level surveillance studies to monitor equitable healthcare access.
Highlights: Poverty and hardship financing are highly prevalent among NCD patients in rural Haiti.Patients attending clinic are less poor than expected from the community.People travelling farther to clinic are less poor.Socioeconomic data should be collected to monitor healthcare access equity.
Keywords: diabetes; equity; global health; hypertension; noncommunicable disease; poverty.
Copyright: © 2020 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures




References
-
- GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392: 1859–922. DOI: 10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- Blot V, Cayemittes M, Charles E, et al. Enquête Mortalité, Morbidité et Utilisation des Services (EMMUS-VI) 2016–2017 Pétion-Ville, Haïti; 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
