

Heart Rate Variability, HIV and the Risk of Cardiovascular Diseases in Rural South Africa
- PMID: 32489790
- PMCID: PMC7218774
- DOI: 10.5334/gh.532
Heart Rate Variability, HIV and the Risk of Cardiovascular Diseases in Rural South Africa
Abstract
Background: Antiretroviral therapy (ART) transformed human immunodeficiency virus (HIV) infection into a chronic disease. Possible HIV-associated complications have emerged including cardiovascular diseases (CVD).
Objectives: This study aims to determine the heart rate variability (HRV) distribution and association between HRV and HIV treated with ART in a rural African population.
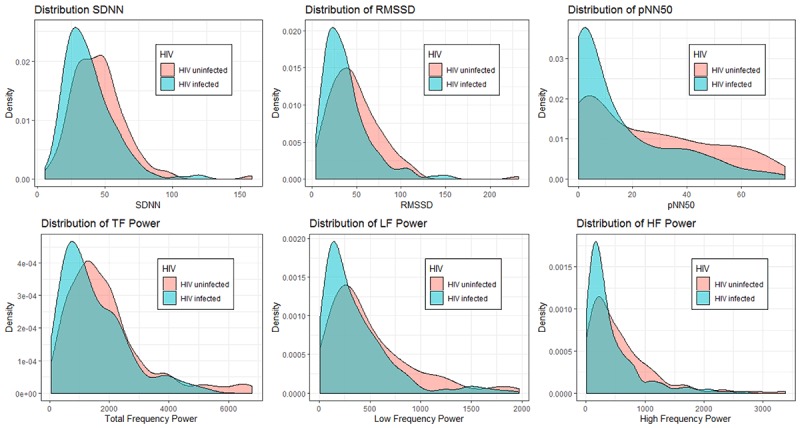
Methods: This cross-sectional study included 325 participants of the Ndlovu Cohort Study, South Africa. HRV was measured using a standardized five-minute resting ECG and assessed by the standard deviation of normal RR intervals (SDNN), root of mean squares of successive RR differences (RMSSD), percentage of RR intervals greater than 50 milliseconds different from its predecessor (pNN50), total-, low- and high-frequency power. CVD risk factors were assessed using measurements (blood pressure, anthropometry, cholesterol) and questionnaires (e.g. socio-demographics, alcohol, smoking, physical activity, age, diabetes). We used a Wilcoxon rank test to assess differences in medians between HIV-infected and HIV-uninfected participants and multivariable linear regression to investigate associations between HRV and HIV treated with ART.
Conclusions: Of the participants, 196 (61.4%) were HIV-infected treated with ART and 123 (38.6%) were HIV-uninfected. HIV-infected consumed less alcohol, 52% versus 35%, smoked less, were less physically active, more often attained lower education, 26% versus 14%, and had lower systolic blood pressure, 134 mmHg versus 140 mmHg, compared to HIV-uninfected. Medians of all HRV parameters were lower for HIV-infected participants. The model fully adjusted for CVD risk factors showed a significant inverse association between HIV treated with ART and log RMSSD (-0.16) and log pnn50 (-0.61). Although HIV-infected participants treated with ART presented with less CVD risk factors they had a lower HRV indicating an increased risk of CVD.
Highlights: - African HIV-infected participants on ART had less conventional CVD risk factors than HIV-uninfected.- However, HIV-infected participants had lower HRV than HIV-uninfected participants.- Lower HRV of the HIV-infected participants indicates that they are at a higher risk for CVD.
Keywords: HIV; antiretroviral treatment; cardiovascular disease; heart rate variability; sub-Saharan Africa.
Copyright: © 2020 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
-
- World Health Organization. Antiretroviral therapy coverage. Data and estimates by WHO region 2018 [cited 31st of Oktober 2019]; Available from: http://apps.who.int/gho/data/view.main.23300REGION?lang=en.
-
- World Health Organization. Prevent HIV, test and treat all – WHO support for country impact. 2016. Contract No.: WHO/HIV/2016.24.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
